Spoke fracture, radius fracture, wrist fracture
Synonyms
radius = Radial bone of the forearm
- Broken spoke
- Radius break
- Base radius fracture
- Radius extension fracture
- Radius flexion fracture
- Broken wrist
- Colles fracture
- Smith fracture
definition
Distal radius fractures are distal fractures of the spoke bone and are usually the result of a fall on the wrist.
The broken spoke is the second most common fracture after the broken collarbone of the human body.

causes

The distal radius fracture near the wrist at a typical location (loco typico) is the most common Broken bone of humans in general (approx. 20-25% of all fractures).
The causes are falls with the attempt to "catch" on most of them stretched (extended), less often bent (flexed) wrist.
The vast majority of the radius extension fracture (Fall on the extended wrist, approx. 85% of all radius fractures) occurs when the wrist is extended between 40 and 90 degrees. If the wrist is extended even more, the carpal bones are more likely to be injured, while if the wrist is less extended, the forearm or elbow is often injured.
If the wrist is flexed, the wrist-near radius flexion fractures occur. Older people with poor bone substance are more often affected (osteoporosis).
The reasons why patients fall are of course very different. In summer it is often the trend sports such as skateboarding or inline skating that lead to broken spokes near the wrist, in winter black ice plays the greatest role.
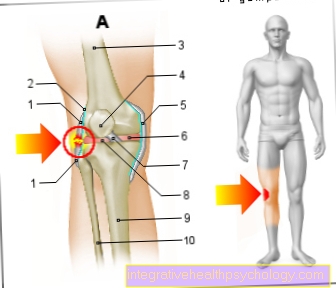
Figure spoke

- Spoke shaft -
Corpus radii - Ellschaft -
Corpus ulnae - Upper arm shaft -
Corpus humeri - Upper spoke ellipse
Joint -
Radioulnar articulation
proximalis - Lower spoke-ellbow
Joint -
Articulatio radioulnaris distalis - Roughness of the spoke -
Radial tuberosity - Spoke neck - Collum radii
- Ring band of the spoke -
Annular radii ligament - Spoke head - Caput radii
- Interbone membrane -
Membrana interossea antebrachii - Stylus process of the spoke -
Radial styloid process
You can find an overview of all Dr-Gumpert images at: medical illustrations
Appointment with ?

I would be happy to advise you!
Who am I?
My name is I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
In order to be able to treat successfully in orthopedics, a thorough examination, diagnosis and a medical history are required.
In our very economic world in particular, there is too little time to thoroughly grasp the complex diseases of orthopedics and thus initiate targeted treatment.
I don't want to join the ranks of "quick knife pullers".
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You will find me:
- - orthopedic surgeons
14
You can make an appointment here.
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
For more information about myself, see - Orthopedists.
classification
The simplest and most common division is that of:
- Radius extension fractures (Colles fracture = Colles fracture): Fall on the extended wrist.
- Radius flexion fractures (Smith fracture = Smith fracture): Fall on the flexed wrist
It is only a rough fracture classification that leaves many therapy-related questions unanswered.
The generally recognized and widely used AO classification is more detailed, but also more complicated:
Classification of distal radius fractures
A fracture: radius fracture / spoke fracture without involvement of the wrist
- A1 fracture of ulna (ulna), radius (spoke) intact
- A2 fracture of the radius, simple and impacted
- A3 fracture of the radius with multiple fragments
B fracture: radius fracture with partial wrist involvement
- B1 fracture saggital fracture
- B2 fracture dorsal fracture
- B3 fracture volar fracture
C-fracture: radius fracture with wrist involvement (articular)
- C1 fracture articular simple, metaphyseal simple (metaphyseal = shaft area near the wrist)
- C2 fracture articularly simple, metaphyseally multi-fragmentary
- C3 fracture articular and metaphyseal multi-fragment
With this classification, all distal radius fractures can be mapped and specific therapy decisions can be derived.
Read more on the topic: AO classification
Symptoms and ailments
The doctor faces the classic picture of a distal radius fracture (trade fracture) as follows:
- swelling
- Pain, tw. Pain in the navicular bone
- Misalignment (this allows conclusions to be drawn about the injury mechanism and severity)
- Functional restriction (functio laesa) = restricted mobility
The affected wrist is presented by the patient in a relieving posture, an actual movement in the wrist no longer takes place (Functio laesa).
On closer inspection, the wrist is swollen and in the case of a very displaced injury, there is one Bayonet misalignment of Wrist before, i.e. the broken spoke near the wrist has shifted towards the back of the hand and at the same time towards the spoke, creating the typical image of a bayonet position of the forearm.
On the Broken bone (Fracture) can trigger sensitive pressure pain. Any attempt to move the wrist is felt to be extremely painful, and often it can produce rubbing noises from the broken bone (Crepitations).
Duration
Depending on the form of therapy, a different healing time can be expected:
Before any therapy, the broken pieces of Bone back into hers original position to be brought. To set the fragments back up, a local anesthetic (Local anesthetic) injected into the fracture gap. Afterwards it will be through Pull on your fingers and pull on your arm restored to its original position.
Are the fragments not postponed can direct a plaster that the fraction for at least six weeks stabilized. Since the fracture can subsequently shift, the position must be examined in regular X-ray controls. To avoid stiffening, you should still rest Finger exercises and Muscle exercises be performed.
When moving the fraction, operations are required that differ depending on the degree of displacement:
Is the broken spoke only shifted slightly and the Joint not involved, suffice Chimney wires (Kirschner wires) for stabilization. After setting up the break, these will be over small incisions in the skin attached in the bone. This can outpatient be performed. Afterwards, the spoke has to be broken by a plaster at least six weeks be splinted. A subsequent postponement cannot be ruled out here either. After the six weeks, the Wires removed under local anesthesia.
Is the Broken spoke unstable or that Joint also affected, are so-called Plate fixation. These are small ones Metal platesthat are to the bone with Nails or Screws attached. If the spoke breaks, this plate is mainly attached on the flexor side. A Irritation (irritation) of tendons occurs more often with track-side metal plates, which is why the track-side position is avoided. Due to the plating, the arm can Moved again early and a stiffening or muscle breakdown can be counteracted by physiotherapy. This is also known as Exercise stability.
The Removal of the plates is not necessary and another painful treatment can be spared the patient.
Healing with perspective / prognosis
The forecast of the cure depends crucially on the fracture shape of the Radius fracture, fracture management and follow-up treatment (physical therapy) from.
Good results can only be expected if it is possible to set up the fracture steplessly and to create stable conditions in the fracture area. Otherwise it can lead to false joint formation (insufficient stability) and wrist arthrosis (pre-arthrosis due to joint step).
The consequences would be pain, restricted mobility and loss of function of the wrist with effects on the whole arm.
In principle, extensive wrist injuries exist even with optimal therapy worse prognosis than with uncomplicated distal radius fractures. A uncomplicated spoke breakage usually heal without consequences.
complication
Complications can occur in both conservative and surgical therapy.
Complications with conservative therapy:
- Slipping of the fracture (secondary dislocation)
- Pressure damage from plaster of paris
- False joint formation (pseudarthrosis)
- Sudeck's disease
Sudeck's disease, also known as CRPS, is one of the most feared complications of the Wrist fracture.
Complications with operative therapy:
- Vascular, tendon and nerve injuries
- infection
- (Slipping of the fracture)
- Implant loosening
- False joint formation (pseudarthrosis)
- Sudeck's disease
A Mobus Sudeck or CRPS occurs much more frequently after surgical treatment than after plaster therapy.
In principle, however, it is not possible to differentiate whether the rupture (violence) or the operation triggered the CRPS.
Broken spoke in children
The Radius fracture can in any age occurrence. However, there is an accumulation between the ages of six and ten years. Forearm fractures are among the most common fractures in children with around 25%. In children, it gets through in most cases Falls while exercising like playing handball, skateboarding or snowboarding to a broken spoke.
Since the bone in children is still developing and the bone mantle is relatively soft, a so-called Greenwood fracture exist. Here is the one bone broken, the Periosteumthat surrounds the bone, however undamaged. The name greenwood fracture comes from the observation of a green twig that may have broken inside, but is still encased on the outside by an undamaged bark. This type of broken spoke occurs especially in children because their bone mantle is flexible and so the risk of breakage is reduced.
In children the therapy far more often conservative than in adults. The undamaged periosteum stabilizes the fracture and conservative therapy with a three to four week plaster application is usually sufficient. After the cast has been removed, although the fracture has healed, a Misalignment represent.If this is not too big, there is one spontaneous self-correction possible. A prerequisite for conservative therapy is a Contact of the break ends and a certain misalignment that cannot be exceeded. If the misalignment is too large or if it is completely displaced here, too Chimney wires used.
The Healing prognosis is here due to the spontaneous healing tendency in children very good. There is controversy as to when the Need for surgical therapy given is. It should be remembered that metal plates are often not necessary for children and that these are more stressed by the additional procedures such as anesthesia and the procedure itself.





















.jpg)