Aortic tear
introduction
The aorta is the main artery and runs from the heart towards the legs, where it then splits.
A tear in the aorta is life-threatening as even a small tear can lead to mass bleeding in seconds. The rupture of the aorta is relatively rare, it is given in the literature with about 5 / 100,000. However, this number only refers to the aortic tears caused by aortic aneurysms. Aneurysms are defects in the vessel wall that can lead to bulging of the vessel or to holes, so-called perforations, in the vessel wall. Aortic ruptures caused by accidents are therefore not listed in the literature.

Classification of an aortic tear
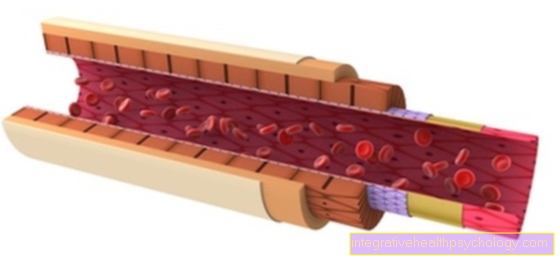
The aorta (main artery) is a vessel made up of three different layers. These layers are made up of elastic fibers, connective tissue and muscle cells. However, these layers can separate from each other due to various triggers. This splitting is described in the specialist literature as a dissection.
In addition, the aorta can be divided into different sections. For example, this can be divided into an upper and a lower section. The upper section is near the heart, while the lower section is remote from the heart. Depending on the area in which the dissection is located, it is divided into different types.
Read more on this topic at: Aortic dissection
Type a
A type A aortic dissection is a tear in the vessel wall in which the entry opening of the tear is in the first section of the aorta (so-called. Ascending aorta) is located. As a result, this rift is located near the heart.
Type A dissection is an acutely life-threatening condition and various consequential damage to the heart can occur within a short period of time.On the one hand, the vascular wall tear can spread to the coronary arteries and thus lead to a heart attack. On the other hand, it can lead to a sudden terminal disorder of the aortic valve (Aortic regurgitation) come, which can also be fatal.
Therefore, imaging should be done as soon as possible if an aortic injury is suspected. If an aortic dissection of type A is diagnosed, emergency surgery must be initiated immediately to attempt to replace the affected section of the aorta with a vascular prosthesis. Despite measures taken in good time, the risk of a fatal outcome is high.
Read more on the subject at: Aortic dissection type A
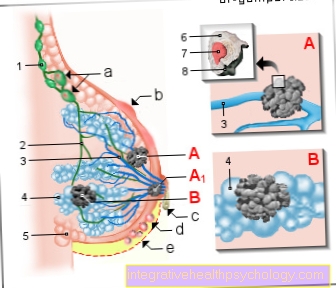
Illustration of an aortic tear

The aortic tear
- Aortic arch - Arcus aortae
- Ascending aorta -
Ascending aorta - Thoracic aorta
(descending aorta) -
Thoracic aorta - Diaphragm -
Diaphragm - Abdominal aorta -
(above the renal artery)
Abdominal aorta - Left kidney - Ren sinister
- Abdominal aorta
(below the renal artery)
Abdominal aorta - Aortic fork - Bifurcatio aortae
- Adventitia -Tunica adventitia
- Media -Tunica media
- Intima - tunica intima
A - aortic dissection
a - Structure of the aortic wall
(9.-11.)
b - Hemorrhage after intimacy
c - Intimar tear after media bleeding
B - aortic aneurysm
d - Thoracic aorta
e - Abdominal aorta
f - Thoracoabdominal aorta
You can find an overview of all images from Dr-Gumpert under: medical images
Type B
A type B aortic dissection is present if the aortic tear in the vessel wall lies below the vascular outlet of the left clavicular artery. This means that, unlike type A, this crack is remote from the heart.
Emergency surgery is only indicated in rare cases in type B. First of all, an attempt is made to keep the patient's condition stable through medicinal measures and close-knit clinical controls. After further diagnostic measures, the torn aortic wall can then be stabilized by a planned open operation or by a vascular stent that is advanced through an inguinal artery.
The aortic aneurysm
A Aortic aneurysm describes a vascular sac in the main artery. This bulge is caused by a widening of the vessel wall, as the different layers that make up the vessel wall are weak in this area. Above all, the elastic fibers and muscle cells that give the vessel stability are displaced.
As a result, the vessel continues to expand over time until a bulge develops, which is associated with a risk of rupture.
Risk factors that favor the development of an aneurysm are, for example, high blood pressure, nicotine consumption and hereditary factors.
There are three different types of aneurysms:
- Aneurysm verum
- Falsum aneurysm and
- Aneurysm dissecans
The last form is actually not classified as an aneurysm in medicine.
If the aneurysm has a critical diameter, the risk of an aortic rupture increases, so surgery may be recommended. If an aortic rupture occurs through an aneurysm, life-threatening internal bleeding can suddenly occur, and there is only a chance of saving the patient's life through immediate surgery.
Read more on this topic at: Therapy of an aortic aneurysm
causes
There are two causes of an aorta rupture. In principle, accidents can tear the aorta, but this is extremely rare because the aorta is relatively protected in the body. A much more common reason for the aorta rupture is an aortic aneurysm.
An aneurysm is an enlargement of a vessel. If the vascular wall is stretched more and more, it can tear. Since several liters of blood flow per minute in the aorta, a person can bleed to death very quickly through a tear in the aorta.
The causes of these aneurysms are different. Aneurysm can result from:
- very high blood pressure (which has persisted for a long time)
- Infections
- Connective tissue diseases such as Ehlers-Danlos syndrome
- Inflammation
However, the greatest risk factor is arteriosclerosis.
However, if aneurysm is present, it is very rarely noticed. An aneurysm does not cause pain and has very few symptoms. Most often, it is found by chance during health checkups.
In Germany there is no preventive medical check-up for aneurysms, even if this has been available for a long time in the USA and Great Britain and has achieved good results and is quite cheap at only about 30 euros.
Read more on the topic: Aortic dissection
Inheritance
If an aortic tear is based on an aortic dissection, there are various risk factors that are inherited in the family. One of the main risk factors is a weakness of the media, i.e. the middle layer in the wall structure of the aorta, and arteriosclerosis. Such a structural weakness of the media occurs, for example, in hereditary diseases such as Marfan syndrome or Ehlers-Danlos syndrome. Increased blood pressure (hypertension) is considered a risk factor for aortic dissection. Genetic factors also play a cause in arterial hypertension. So you can only find a few risk factors that have a familial accumulation or are hereditary and thus increase the risk of an aortic dissection and thus possibly an aortic tear.
In the event of an aortic rupture following trauma or accident, no hereditary risk factors can be found.
Symptoms
Symptoms of an aortic tear differ depending on the type of tear. In the following a distinction is made between a crack (Rupture) which resulted in a Aortic dissection happens and a traumatic injury to the aorta, for example as a result of an accident.
If the vascular wall ruptures as part of an aortic dissection (splitting of the wall layers of the aorta), then acute, suddenly onset and usually stabbing pain dominates, which can radiate into the back area. In addition, there is massive blood loss with the blood flowing into the abdomen or the chest. This results in a drop in blood pressure and the signs of hypovolemic shock. These are a systolic blood pressure (upper blood pressure value) of less than 100 mmHg to less than 60 mmHg, hardly palpable pulses, shallow and faster breathing up to and including impaired consciousness and loss of consciousness. Death by bleeding to death can occur very quickly.
If the tear of the aorta is covered as a result of an aortic dissection, which means that the blood cannot flow freely into the abdominal cavity, this leads to a pulsating and painful mass (tumor), which, depending on the patient, can also be felt from the outside. Here, too, pain that radiates to the back can predominate.
As a result of a rupture of the aorta, draining vessels can be blocked or severed. This leads to an insufficient supply of other organs. These shortages can also lead to neurological failures or a stroke. Neurological failures become noticeable through paralysis or a loss of sensitivity, for example the perception of touch. This type of sleep attack is known as one ischemic infarctionbecause it occurred as a result of insufficient blood supply to the brain or parts of the brain. Likewise, abdominal pain (no supply of the relevant arteries to organs of the gastrointestinal tract) or acute kidney failure (Renal arteries no longer carry enough blood) occur.
The bleeding from the aortic tear also leads to weakened or laterally unequal pulses in the legs and feet or arms and hands in the further course of the vessel.
If the aortic tear is very far in the upper part of the aorta, i.e. close to the exit of the aorta from the heart, a tear can also involve the heart. Symptoms of aortic valve insufficiency (the aortic valve of the heart no longer close properly) or pericardial effusion dominate here the one for a heart bag tamponade can lead. Aortic valve insufficiency means that in the filling phase of the left heart ventricle the ventricle is not sufficiently sealed to the aorta and there is a return flow of blood from the aorta into the heart. A pericardial effusion is the accumulation of fluid (here blood) in the pericardium. This constricts the heart in the pericardium and it can no longer work properly (Pericardial tamponade). It can lead to shortness of breath and reduced performance.
If an aortic tear occurs after a traumatic event such as an accident, the symptoms of the accompanying injuries usually dominate. Patients with a traumatic aortic tear are mostly polytraumatic Patients, this means that they have multiple, mostly life-threatening injuries. Here, too, pain can occur in the chest and abdominal area, but this does not always necessarily come from the aortic tear due to the polytraumatic injuries.
Due to the massive blood loss, in which, depending on the type of injury, the blood can flow into the abdominal cavity or, in the case of open injuries, outwards, it can also lead to hemorrhagic conditions here shock come. This means shock symptoms due to the lack of volume due to blood loss. Tachycardia dominates the shock (increased heart rate), a hypotension (Blood pressure values below 100/60 mmHg) and dyspnea (difficult breathing up to breathlessness).
Signs of a ruptured aorta
The first signs of an aortic rupture or aortic dissection are sudden pain.
This pain is usually classified as very extreme, described as stabbing and usually migrates from the crack location towards the back.
The severe blood loss can lead to symptoms in a very short time. If, for example, the characteristic pain sets in and very low blood pressure is measured shortly afterwards, the interplay of these signs can indicate an existing aortic tear.
The loss of blood can also be accompanied by a loss of consciousness because not enough blood is getting to the brain.
In addition to open bleeding in the chest or abdomen, in which the symptoms worsen rapidly, the signs of a so-called covered aortic tear may be different.
The bleeding is suppressed or at least limited by anatomical structures. In contrast to the continuous pain of an open aortic tear, pulsating pain occurs. The bleeding creates a mass that can cause other symptoms in addition to local pain.
If a growing structure near the aorta is felt when the pain is appropriate, this can be a sign of a rupture of the aorta.
You may also be interested in this topic: Symptoms of aortic dissection
diagnosis
The diagnosis of an aortic rupture is not easy to make. If a crack is suspected, however, action must be taken very quickly, as the death rate is very high depending on the size and location of the crack. A tear or expansion of the aorta can be detected by ultrasound, especially by swallowing ultrasound, CT and MRI. X-rays can provide evidence of a crack, but are not suitable for diagnosis.
Read more on the topic: Chest x-ray (chest x-ray)
First aid for an aortic rupture
Surgical intervention is essential for an acute aortic rupture. Therefore, if an aortic rupture is suspected, the emergency call (112) should be canceled immediately, as the patient must be brought to a heart and thoracic surgery clinic / center as soon as possible. However, diagnosing an aortic tear without technical aids (e.g. ultrasound) is difficult, since almost all tears do not arise traumatically but spontaneously.
Until the emergency doctor arrives, the patient should be placed in the stable lateral position in the event of unconsciousness and in the shock position in the event of shock. Provide sufficient warmth or a warming mat, i.e. if possible, cover the patient and do not lay it on a cold stone floor but, for example, on a carpet. The patient should be reassured and sufficient oxygen should be provided (e.g. use of an oxygen probe if one is present due to previous illnesses of the person concerned). Regular pulse and breathing should also be checked until help has arrived. If the cardiac arrest has already occurred, the patient must be resuscitated immediately (cardiopulmonary resuscitation).
Since only an operation can help for hemostatic therapy, the emergency doctor can only treat symptomatically before reaching the clinic. Symptoms such as severe chest / back pain, shortness of breath, unconsciousness, differences in blood pressure in the arms and legs, severe drop in blood pressure up to shock and complete circulatory failure may be present. The most important thing is to relieve these complaints while keeping the circulation stable and relieving pain.
Read more about the topic here:
- resuscitation
- Stable side position
therapy
Depending on the location and size of the aortic tear, there are different therapy options.
The tear can be treated with an operation with a vascular prosthesis, or with the help of a stent, which is inserted with the help of catheters. In addition, the blood pressure is brought to around 110/60 with the help of medication and is closely monitored. The severe pain can be controlled with the help of opiates.
Operation of the aortic rupture
There are two different surgical techniques for treating an aortic tear.
The first technique is open, conventional care. The left chest cavity (thorax) opened (so-called left lateral thoracotomy) if the aortic tear is level with the thoracic aorta. If the aortic tear is more in the area of the abdominal aorta, a longitudinal incision is usually made in the middle of the abdomen or, more rarely, a flank or transverse abdominal incision. The injured part of the aorta is exposed and optionally replaced with a prosthesis or closed with a direct suture. This prosthesis can be called a pipe- or Y prosthesis made of plastic and closes the injured part of the aorta. A Y-prosthesis consists of three connected tubes (Y shape) and is chosen when connected vessels such as the pelvic arteries are also injured and must also be splinted. Otherwise, the simpler tubular prosthesis is chosen.
This type of operation is a high risk for polytraumatic patients, i.e. patients with serious and life-threatening accompanying injuries. The operation takes a long time and is performed under general anesthesia. In addition, only one half of the lung is ventilated during the operation and a connection to a heart-lung machine may also be necessary.
The second technique is that endovascular stent delivery (TEVAR = Thoracic Endovascular Aortic Repair). Here, a computed tomography-assisted Angiography (Representation of the aorta with the help of imaging techniques). This exam can be used to assess the aorta. The appropriate size for a stent is selected. A stent is an expandable tube, which consists of either a metal or plastic braid. Such a stent is inserted into the aorta. This takes place arterially via the arteria femoralis, i.e. the artery on the thigh. Under angiographic control, the stent is advanced over the femoral artery to the aorta and positioned at the tear site. The stent is now seated over the aortic tear. Over time, the endothelium (wall of the aorta) of the aorta can grow over the stent and the closure of the tear and the preserved rag of the aorta are secured.
Under certain circumstances, such an operation can also be carried out under spinal cord or local anesthesia and therefore does not require general anesthesia like an open procedure.
Also read: Aortic prosthesis
Healing time after an intervention
An acute aortic rupture is followed by lengthy intensive care treatment and monitoring.
Sometimes the person concerned has to be kept in an artificial coma so that the body has time to heal. The exact healing time cannot be determined, as this varies depending on the person affected and the type of rupture and therapy. However, it may take a few months for full healing. During this time, the person concerned is not fully physically resilient.
Aortic rupture prognosis
The prognosis depends on many factors.
The larger the crack, the later it is recognized and the less favorable the location, the death rate can be over 80%.
If the aortic tear is treated early, the mortality can drop to 20%.
Life expectancy
The chances of survival in an aortic tear, which usually occurs in the form of a “ruptured (torn) aortic aneurysm” (not to be confused with “aortic dissection”), depend heavily on the location of the tear and the area in which the blood flows.
A distinction is made between covered and free bleeding. With free bleeding, blood flows into the abdominal cavity. Since this can take up a lot of volume, there is an enormous loss of blood within a very short time. With covered bleeding, the blood flows into a space behind the abdominal cavity, the so-called "retroperitoneum". This area can only take up a limited volume, which is why there is less blood loss. In the case of an aortic rupture, only patients with covered bleeding usually reach the hospital alive. This is around 50%. Of these 50%, however, only about 70% make it to the operating room. The survival rate of an emergency operation for a ruptured aortic aneurysm is around 60% and depends on the individual care within the hospital and the experience of the surgeon.
The main problem with patients with a traumatically caused aortic rupture (e.g. as part of an accident) is that these patients are mostly polytraumatically injured. A multiple trauma occurs when there are two or more injuries that are life-threatening. Therefore, the cause of death is usually not even causally the aortic tear. In general, the accompanying injuries determine the prognosis and the course of the aortic tear.
If the aortic tear is the result of an aortic dissection, the prognoses differ depending on the location of the tear. If there is a tear in the aortic arch or even closer to the exit point from the heart (Ascending aorta) the lethality (the probability of dying from the aortic tear) is around 1% per hour in the first 48 hours. The one-year survival rate for this type and location of injury without surgery is 5%. It becomes clear that there is an urgent and urgent need for action here. If an operation was performed on time, the one-year survival probability is 60-80% and depends on the patient's other health.
If the aortic tear is in the descending part of the aorta (Descending aorta), the chances of survival with drug treatment of the aortic tear are 60-80%.
Consequences of an aortic tear
The consequences of an aortic rupture can be devastating.
In most cases, the heavy bleeding initially leads to an insufficient supply of the organs that lie behind the defective area. With increasing blood loss, organs in front of it are also affected because the circulating blood volume is no longer sufficient for supply.
If the tear is very high before the vessels to the head and brain leave the aorta, this can result in impaired consciousness - or loss, neurological deficits or a stroke.
Depending on the severity and duration of the undersupply, permanent consequential damage can arise even if the patient is rescued.
If the tear with the associated bleeding is close to the heart, its function can also be restricted. For example, it can happen that the aortic valve, the heart valve which is located between the heart and the aorta, no longer closes properly, which further reduces the blood flow.
Compression of the heart due to the massive mass or bleeding into the pericardium (Pericardial effusion) interferes with the work of the heart, causes massive pain, shortness of breath and, in the worst case, death of the patient.
An undersupply of the kidneys can lead to acute kidney failure, which after a short time leads to the kidneys stopping their function. If the patient's life can be saved, this results in lifelong renal replacement therapy (dialysis) or the need for a kidney transplant.
The undersupply of organs in the gastrointestinal tract leads to necrosis as a long-term consequence. This means that parts of the intestine die and have to be removed.
Depending on the gastrointestinal section, this means a more or less good prognosis for the patient.
Overall, an aortic tear is to be regarded as extremely problematic in terms of prognosis. Since an aortic tear is almost always associated with massive bleeding, only about half of all untreated patients would survive. However, the death rate can be more than halved through advanced drug therapy and modern surgical techniques. Thus, after one month, around 80% of patients who have suffered an aortic dissection are still alive.
Complications during and after surgery
Emergency surgery for a ruptured aorta is a high-risk operation. Immediately after the operation, there may be a leak in the operated area and consequent bleeding.
The high blood loss that occurs with the original rupture has many consequences. Wound healing is slowed down, the circulation is weakened and the missing white blood cells are also a problem for the immune system. In addition, the blood transports the oxygen in the body and this is only possible if there are enough blood cells. The blood loss also has an effect on the kidneys, which need a certain blood pressure in order to fulfill their filter function. Blood transfusions are therefore often necessary during the operation.
Furthermore, the long length of stay in the intensive care unit can lead to further illnesses. These include pneumonia, pressure sores and thrombosis. A late complication can be the formation of thrombi on the surgical scar, since the blood flow can be changed in the area of the scars.
What do you have to consider for the rest of your life?
To answer this question, it must first be defined whether it is the postoperative course, i.e. the first days and weeks after the operation, or the future life after an aortic rupture.
During the first few days after such an event, it is determined whether other organs have been damaged by the injury. This happens due to the enormous loss of blood, which is associated with an insufficient supply of blood to other organs. The brain, kidneys and intestines are particularly susceptible to this. A simultaneous failure of several tissues, a so-called "multi-organ failure" is also possible.
If the first days and weeks pass without complications, the worst is over and the patient can usually return to his former daily routine. However, regular check-ups should be carried out. How often this is done depends on whether the operation was a minimally invasive or an open procedure. While a follow-up check-up every 2-3 years is sufficient for an open operation, an annual check-up is required for a minimally invasive operation.
Since high blood pressure is an important trigger of aortic aneurysms and thus also of tears, an excessively high blood pressure should be adjusted with medication. Blood lipids and blood sugar also have a major influence on the health and stability of blood vessels. These should therefore also be checked regularly and corrected with medication if necessary. A nutrition plan can also be helpful here, so that certain fats and sugars can be controlled without medication.















.jpg)