End-stage COPD
definition
COPD is a chronic disease that cannot be cured, but can be avoided in many cases by avoiding risk factors. It is classically divided into 4 stages. Here stage 4 is the final stage. The staging is based on various respiratory parameters and the type of accompanying symptoms. The revised stages according to gold nowadays provide a division into stages A to D, where D can be viewed as the final stage. The disease progresses slowly. Switching off the most important risk factor, smoking, in good time can prevent progression or significantly delay it. In addition to the chronic symptoms in the end stage, there may be an additional acute worsening of the symptoms, which is then referred to medically as one Exacerbation.

What are the typical symptoms of end-stage COPD?
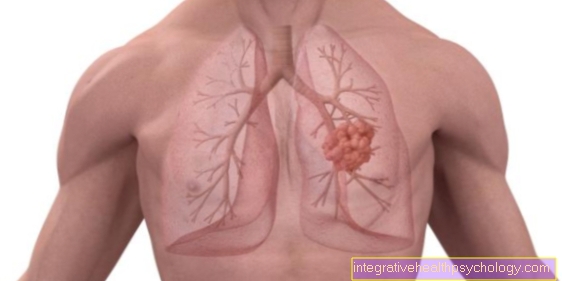
The main symptom of end-stage COPD is severe shortness of breath. In COPD there is an increasing destruction of lung tissue so that from a certain point there is no longer enough lung tissue to ensure an adequate supply of oxygen. This leads to shortness of breath. This is progressive if the causative factors (especially cigarette smoke) are not eliminated. Advanced COPD patients often stand out because they use their auxiliary breathing muscles to get better air. A typical posture here is the so-called coachman's seat. The patient sits with his arms supported on his thighs. Subjectively, this results in a somewhat better ventilation of the lungs. The lip brake is also a method that COPD patients often unconsciously use to reduce the shortage of breath. Here you exhale against your lips, which are slightly on top of each other. While in patients with COPD in the earlier stages often a Exertional dyspnea present, i.e. shortness of breath that occurs during physical exertion, in most cases it is pronounced in end-stage patients Resting dyspnea, i.e. shortness of breath that is already present at rest. Another typical symptom of advanced COPD is a chronic cough. Characteristic of this cough is that it is not a dry cough but that it is accompanied by sputum. The cough is often strongest in the morning hours and is often more pronounced in the autumn and winter months than during the rest of the year.
Read more on the topic: Breathing exercises
What are the signs that the terminal stage has been reached?
The stages of COPD, both in the new and in the old classification, are essentially determined by certain breathing parameters that are determined by a lung function diagnosis. A COPD in stage 4 (old classification) or D (new classification) is only present if certain values are available. In addition, chronic complaints occur in the end stage. So there is permanent shortness of breath with coughing and sputum. The risk of exacerbation is high. The constant occurrence of productive coughing, as well as shortness of breath at rest, and an increased incidence of exacerbations are signs that the end-stage of COPD has been reached.
What can you do about the feeling of suffocation?
In the end stage, COPD (chronic obstructive pulmonary disease) is often accompanied by a subjective feeling of suffocation. This can initially be compensated by a supply of oxygen in higher flow rates. Later on, certain body positions will help to improve breathing.
For example, putting your hands on your legs can improve the work of the respiratory muscles. The lip brake can widen the airways and thus ensure a better situation when exhaling.
In addition, you should no longer sleep completely lying down, but rather with your upper body elevated.
So-called palliative therapy can take place in the absolute final stage. Among other things, drugs are used that have an anxiolytic effect.
What does the therapy look like in the end stage?
The therapy of COPD is based on the stages of the disease. In stage 4 after GOLD, maximum therapy is used. These include inhalative Glucocorticoids (Steroids) in combination with a long-acting Anticholinergic or a long-acting one Beta-2 sympathomimetic. Also Roflumilast, a relatively new active ingredient from the group of PDE-4Inhibitor can be used. Theophylline is also used in some patients. Inhaled glucocorticoids are available in the form of combination preparations with long-acting beta-2 mimetics. Not all COPD patients benefit from glucocorticoid therapy, so that the success of the therapy should be evaluated regularly. If the symptoms do not improve, the therapy should be changed. Glucocorticoids that are frequently used include Budenoside and Fluticasone. Commonly used beta-2 mimetics are Formoterol and Salmeterol. From the group of long-acting anticholinergics are common Ipatropium bromide and Tiatropium bromide used. In the event of an acute exacerbation, the use of antibiotics may also be necessary. However, it is not absolutely necessary and should be carefully considered in each individual case. In patients with end-stage COPD in particular, drug therapy often does not provide sufficient relief from the symptoms. Long-term oxygen therapy is therefore often also necessary. The oxygen is supplied through a nasal cannula. The patients receive a house oxygen device for this. If there is sufficient indication, this will be financed by the statutory health insurance. If the CO2 values in the breathing gases are significantly higher, non-invasive ventilation may also be necessary. This form of ventilation relieves the respiratory muscles and leads to better gas exchange with a sufficient reduction in the CO2 value. This type of ventilation is used both as an acute measure in inpatient everyday life and as home ventilation. The last resort for end-stage COPD is intubation and invasive ventilation in a clinic. A lung volume resection can also be considered. In an endoscopic procedure (bronchoscopy) Valves used in the lungs to counteract the overinflation of the lungs that is typical of COPD. This is not a proper operation, but the procedure is usually performed under general anesthesia.
Can morphine relieve the symptoms?
Morphine belongs to the group of opiates. The drug is now called morphine. It is not an everyday drug in the treatment concept for COPD. Nowadays, however, it is sometimes used as a medicinal last resort during inpatient hospital stays when the acute shortness of breath cannot be managed in any other way. The relief of shortness of breath with morphine is mainly due to the fact that opiates reduce restlessness and anxiety and lead to a decrease in the work of breathing.
What level of care do you get with terminal COPD?
The level of care (or degree of care) is based on six different criteria. Above all, mobility and self-sufficiency in COPD are impaired due to the severe shortage of air in the terminal stage. Social contacts and everyday life also suffer from the disease.
In the final stage of COPD, the patient should be classified in the highest level of care (level 5). However, this classification is often dependent on minor details, so that if the classification is lower, professional help should be sought for the care application.
What are the complications of end-stage COPD?
Since COPD is a serious lung disease, lung-associated complications are usually the most common. This includes the exacerbation of respiratory infections at all stages. With mild colds, the necessary breathing work can no longer be carried out, so that there is increasing shortness of breath. In addition, the pathogens settle much faster than in people with healthy lungs, so that pneumonia often occurs.
These must be treated as an inpatient in the final stage, as they lead to a rapid deterioration in lung function and can therefore be life-threatening. The chronically progressive worsening of the work of breathing also plays a major role in end-stage COPD.
In addition, the overinflation of the lungs can cause the blood to stagnate in the pulmonary vessels and thus overload the right half of the heart.
lung infection
Pneumonia is a typical complication of many diseases of the lungs and respiratory tract. In end-stage COPD, the airways are very susceptible to pathogens, which means that respiratory infections can quickly develop. These spread particularly well to the lungs, where they lead to pneumonia.
The most common pathogens are the bacteria Streptococcus pneumoniae and Haemophilus influenzae, but viruses can also cause pneumonia. As a result, breathing becomes difficult in addition to the already existing shortness of breath in terminal COPD.
This leads to what is known as respiratory failure (inability to take in enough oxygen and release enough carbon dioxide). Therefore, pneumonia in end-stage COPD is a life-threatening emergency that requires intensive care.
The therapy is initially carried out using inhaled substances that widen the airways. In addition, the pathogens (if the pneumonia was caused by bacteria) should be treated with antibiotics. If there is increasing respiratory failure, supportive, non-invasive ventilation is carried out first. In an emergency, invasive ventilation is also possible. Other complications such as the presence of severe cardiac stress must also be taken into account during therapy.
water in the lungs
In the final stage of COPD, so-called "air-trapping" occurs. The air you breathe in cannot be completely exhaled due to the narrowing of the airways, so that the air is trapped in the lungs. If this (or other mechanisms such as the collapse of airways or infections in the lungs) damage the lung tissue, the body starts an immune reaction.
This is accompanied by the release of inflammatory cells and fluid. This fluid collects in the lungs in the form of water. In addition, COPD causes the blood vessels in the lungs to constrict. This increases the pressure, especially in the right side of the heart, and can worsen the buildup of water in the lungs.
What is the end-of-life expectancy?
Life expectancy in end-stage COPD depends on other factors such as the presence of other medical conditions and the presence of risk factors (such as continued nicotine use). The success of the therapy also plays a decisive role. The occurrence of exacerbations also plays a decisive role in the question of life expectancy. Repeated exacerbations in the end-stage of COPD can be life-threatening and fatal. The life expectancy of end-stage COPD cannot be given a generalized estimate due to the factors mentioned above.