Heart muscle
definition
The heart muscle (Myocardium) is a special type of muscle that only occurs in the heart and forms the majority of the wall of the heart. Due to its regular contraction, it is responsible for the fact that the blood is pressed out of the heart (the heart's job) and is pumped through our body and is therefore vital.
Structure of the heart muscle
The heart muscles own properties of both smooth and striated muscles and is therefore a special form.
In terms of structure, it corresponds more to the striated, i.e. the skeletal muscles.
The single ones muscle fibers are structured here in such a way that the Proteins, which are responsible for the contraction, the actin and the myosin, are arranged so regularly that this special structure ensures that the cells under polarizing light a kind of Horizontal stripes exhibit.
That too Tubule system (membrane-bounded spaces within the cytoplasm, which are called Calciumstorage and thus play an extremely important role in the contraction of the muscle) is similar to that of the striated muscles, which is why the heart is just as capable of this as the skeletal muscles quick and above all powerful contraction to reach.
A feature that the heart muscle cell (cardiomyocyte), on the other hand, shares with the cells of the smooth muscles has in common is that each cell has its own nucleus which is usually located in the center of the cytoplasm. Only rarely are there two nuclei per cell, whereas there can be hundreds in a skeletal muscle cell. Therefore, in contrast to the striated muscle cells, one speaks here of only one "Functional" syncytiumbecause the cells are closely coupled but not fused together.
In addition, there are properties that only the heart muscles have: An important feature is, for example, that the individual heart muscle cells are connected to one another via so-called glossy strips (disci intercalares). On the one hand, these glossy strips contain desmosomes and adherence contacts. Both of these structures contribute to the stabilization of the cell structure and the transmission of forces between the individual cells. On the other hand, there are also gap junctions in the glossy strips, i.e. practically small “gaps” between neighboring cells, through which an ion flow and thus an electrical coupling is possible.
Conduction and contraction
The electrical excitation of the heart muscle occurs through a intrinsic conduction system, which, as with smooth muscles, is based on the presence of itself spontaneously discharging (depolarizing) Pacemaker cells is based.
The first instance of this system is the so-called Sinus node, the primary pacemaker. Here is the Heart rate in healthy people with about 60 to 80 beats per minute. The excitation is transmitted from the sinus node to the Muscles of the two atria.
These contract and pass the excitement on to the AV nodelocated between the atria and the ventricles. After a moment's delay in the excitement in this, it eventually becomes over that Bundle of his, the Tawara thigh and ultimately the Purkinje fibers on the Heart muscle of the ventricles transfer.
This forwarding also takes place via Gap junctions and not via special nerve fibers. As a result of the excitation, the heart chambers then contract and thus empty the blood remaining in them into the adjoining vessels.
So you can differentiate between two different phases with each heartbeat: diastole, in which the heart muscles of the chambers relaxed and the cavities fill with blood. This is always followed by the Systole, in which the muscle cells of the heart chambers are tense and build up such a high pressure that the blood can eventually be pumped out of the heart.
Should there be short-term fluctuations in blood pressure (for example, if you suddenly stand up after lying down for a long time and the blood pressure suddenly drops relatively sharply because the blood initially sinks into the legs), the heart muscle can generally adapt its activity itself first without having to the brain stem or the autonomic nervous system must be switched on. This is done by the so-called Frank Starling mechanism, which is based on the pre-filling of the heart and the afterload, i.e. the pressure in the downstream vessels into which the blood is to be pressed.
Properties of the heart muscle
In humans, a heart muscle cell is on average about 50 to 100 µm long and 10 to 25 µm wide. The left ventricle is the chamber from which this Blood in the circulatory system is ejected.
This must therefore be a much higher pumping power provide than that right ventriclethat only the lung supplied with blood.
Therefore, the heart muscle of the left ventricle is usually also an inch about twice as thick like that of the right ventricle, which is usually only about 0.5 cm thick.
It is believed that at the beginning of our life there are up to 6 billion cells in the muscles of the left ventricle. However, this number then steadily decreases in the course of life, so that presumably only a number of two to three billion cells can be detected in older people.
Illustration heart
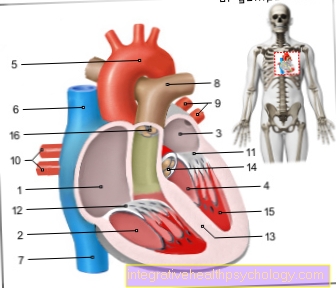
- Right atrial -
Atrium dextrum - Right ventricle -
Ventriculus dexter - Left atrium -
Atrium sinistrum - Left ventricle -
Ventriculus sinister - Aortic arch - Arcus aortae
- Superior vena cava -
Superior vena cava - Lower vena cava -
Inferior vena cava - Pulmonary artery trunk -
Pulmonary trunk - Left pulmonary veins -
Venae pulmonales sinastrae - Right pulmonary veins -
Venae pulmonales dextrae - Mitral valve - Valva mitralis
- Tricuspid valve -
Tricuspid valva - Chamber partition -
Interventricular septum - Aortic valve - Valva aortae
- Papillary muscle -
Papillary muscle
You can find an overview of all Dr-Gumpert images at: medical illustrations
Wall layers of the heart
The heart muscle is that middle of three layersthat actually form the heart. Right on the inside is the so-called Endocardium, from which, for example, the heart valves eversion. That follows Myocardium, so the muscle layer, and on the outside there is still that Epicardium.
This is due to Pericardium, the Pericardium, which surrounds the entire heart and, with the help of the small amount of fluid that is in it, functions as a kind of "shock absorber" and can protect the heart to a certain extent from external vibrations and friction.
Heart muscle diseases
Heart muscle disorders (Cardiomyopathy) can more mechanical, electrical or mixed Be kind. The term mechanical diseases of the heart muscle means a change in the size of the heart, the wall thickness and / or a change in the cavities (atria and ventricles), so that pumping disorders arise. At electrical malfunctions the transmission of electrical potentials is impaired, so that the heart does not work physiologically. As a rule, diseases of the heart muscle are often accompanied by an enlargement of the muscles. Several forms of diseases of the heart muscle are subdivided.
- Thickening of the heart muscle
As a rule, this comes about when there is a in the body's circulation high blood pressure prevails. In response, the left ventricle has to work harder to build up pressure high enough to still eject blood. As a result, more cells are formed and the heart muscle becomes thicker in order to be stronger. However, this only works up to a certain point, from which the muscle is too thick to still be able to be adequately supplied with blood. Then the muscle can no longer work adequately and a Heart failure (Heart failure). In addition, there is an increased risk for you due to the insufficient supply of certain muscle areas with oxygen Heart attack.
- Wearing out the heart muscles (Dilated cardiomyopathy)
In this form of the disease of the heart muscles, the heart chambers enlarge, without an increase in muscles, with reduced ejection capacity. The heart muscles usually increase in size on the left (sometimes also on the right), which means that the heart is no longer able to pump enough blood from the chambers into the bloodstream. The chambers are worn out and there is no strength to expel the blood.
Furthermore, there may be a limited relaxation phase of the heart, this phase being delayed, with the result that the heart becomes increasingly stiff, that is, it loses its elasticity. This promotes deposits of lime in the vessels, which in turn can lead to serious secondary diseases. At the onset of this disease it can be too Shortness of breath come under stress, later even without stress. Furthermore are also Arrhythmia likely in the further course.
- Disease of the heart muscle due to an increase in musculature (Hypertrophic cardiomyopathy)
This leads to an increase in the heart muscles locally in the area of the ventricular septum in the left ventricle. A distinction is made between two forms of the disease in which the outflow tract to aorta, so in the great body circulation, narrowed (severe course) or free (milder course) can be. It is believed that this type of heart muscle disorder is congenital. Young male patients with a family history of sudden cardiac death are suspected to be at high risk, as this disease of the heart muscles is inherited.
- Reduced ductility of the chambers (Restrictive cardiomyopathy)
This form of heart muscle disorder is relatively rare and can be acquired over a lifetime and / or be congenital. How this form is acquired has not yet been clarified. In this disease, the left ventricle is mostly less flexible, but the right ventricle can also be affected in some cases.
At the onset of the disease there is an enlargement of the atria and symptoms of a Heart failure such as shortness of breath. The innermost layer of the heart muscle thickens in the course of the disease and there is an increasing disruption of the relaxation phase of the heart due to the reduced flexibility of the heart muscles.
- arrhythmia the right ventricle (Arrhythmogenic right ventricular cardiomyopathy)
The cause of this heart muscle disease is still unclear. Adipose tissue and connective tissue are deposited in the muscle tissue of the heart muscles. This affects the right ventricle of the heart. Since this form is usually associated with an intact pumping capacity, the disease can progress undetected and severe cardiac arrhythmias can develop over time. The electrical potentials are not passed on sufficiently or irregularly. The heart beats irregularly. Especially young men, especially athletes, are at risk of sudden cardiac death with this disease. The cause is suspected to be gene mutations in various structures that enable the heart muscle cells to communicate with one another, as well as a defect in a receptor in the heart's calcium stores.
- Myocarditis (Myocarditis)
In this form of the disease, there is inflammation of the heart muscles. The inflammation can affect the heart muscle cells, the tissue between the layers of the heart muscles, as well as the Heart vessels affect. A distinction is made between chronic and acute inflammation, depending on the course. The inflammation can be caused by simple infections like that Flu virus or bacteria, toxic substances such as alcohol (very common) or heavy metals, fungi and parasites, drugs or autoimmune reactions are triggered. It is not uncommon for an unclear cause to exist.
The extent of myocarditis depends on the course of the disease. This can be without symptoms, but it can also be accompanied by acute heart failure. Cardiac arrhythmias, Chest pain, Shortness of breath, as well as tiredness, general malaise and fever could be signs of heart muscle disease, particularly inflammation. The chronic form is often symptom-free, in contrast to the acute form. But even in the acute form, the course depends on the severity of the inflammation.
- Stress cardiomyopathy (Tako Tsubo cardiomyopathy)
This is a rare heart muscle disorder that is common in women menopause concerns. It is usually triggered by strong emotional events and symptoms of an acute myocardial infarction occur. Chest pain, anxiety as well as sweating and severe paleness are possible symptoms. Due to the high level of stress, there is an increased release of adrenaline, whereby heart muscle cells are disturbed in their function.
- Cardiomyopathy before or after pregnancy (peripartum cardiomyopathy)
This form of the disease is one through strong Pregnancy stress triggered dilated cardiomypathy (see above). It can occur between the last trimester and five months after giving birth. The causes of this disease have not yet been established.
Strengthen / train the heart muscle

In order to strengthen the heart muscle, it is important not to overload it. In the case of known cardiovascular diseases, it is advisable to discuss the training units with a cardiologist or, if necessary, to carry them out under inpatient supervision.
The heart muscles can be strengthened with light endurance sports and further trained by increasing them, such as walking, inline skating, swimming, cycling or cycling on a recumbent bike. A training session should last at least 20 minutes at intervals (15-17 minutes for beginners and those returning to the sport); if the training level is medium to good, the interval can be increased to 45 minutes. It is important that you check your pulse while exercising, for example with a heart rate monitor or by feeling your pulse on your wrist with two fingers. The resting heart rate of a healthy person (untrained state) is approx. 60-70 heartbeats per minute (60-70 / min).
During endurance training, the heart rate should generally be not over 135 / min climb. It is advisable to have your maximum heart rate determined under medical supervision in order to strengthen your heart if you are training in the optimal range. This is approx. 60% -75% of the maximum cardiac output. Strong press breathing, for example when doing strength training with weights or strong resistance when cycling (only uphill), should be avoided. You should train 3-5 times a week, at the beginning 15-20 minutes at about 60% of the maximum Heart rate. In order to strengthen the heart muscle, the training is gently increased to up to 75% for longer training units.
Heart muscle thickened
If the heart muscles thicken, this is often a consequence of chronic overloading of the heart. Is it said that the heart muscle is thickened (hypertrophy), usually the left ventricle is meant. This is usually between 6 and 12 millimeters thick. Due to chronic overload at, for example high blood pressure, the heart must always expel blood from the left ventricle against much greater resistance in the aorta than it normally would. As a result, the heart adapts to the higher resistance and its muscle cells begin to grow (no reproduction of the individual cells) in order to apply more force and the heart muscle thickens. The more the heart muscle thickens, the less volume the left ventricle can take up from the left atrium.
In most cases there is enlargement of only one side of the heart (asymmetrical), which leads to a disturbed pumping process. The left ventricle is now filled with blood more quickly because its radius is smaller compared to the right ventricle, but it contains less blood and loses its elasticity as it grows. This means that it ejects less blood into the body's circulation per stroke. On top of that, larger muscle cells need more oxygen, which increases the risk of a Oxygen deficiency increases and thus the risk of heart attack also increases.
The thickening of the heart muscle as a result of high blood pressure must be differentiated from the thickening due to heavy physical exertion. The entire heart (not just the left ventricle) grows and the cardiac output increases with a secure oxygen supply.
.jpg)





















.jpg)