ISG - The sacroiliac joint
Synonyms in a broader sense
Medical:
- Articulatio sacroiliaca
- Sacroiliac joint
- Sacrum and iliac joint
- SIG (sacroiliac joint)
Illness:
- ISG blocking
- Scroiliitis
Explanation
The ISG (medical: Articulatio sacroiliaca) is the articulated connection between the sacrum (Os sacrum) and the iliac bone (Os Ilium).
The joint surfaces (facies auricularis) between these two bones are boomerang-shaped to C-shaped and are located between the 1st and 3rd sacral vertebrae.
They consist of an upper and lower pole, the transition point of which is approximately at the level of the 2nd sacral vertebra (part of the sacrum). There is a kink between the upper and lower pole, the angle of which is 100-120 °.
Figure ISG - joint

- Sacrum-iliac joint
(Sacroiliac joint, abbreviated ISG)
Articulatio sacroiliaca - Iliac bone -
Os ilium - Sacrum -
Sacrum - Anterior sacrum-iliac bone
-Tape -
Lig. Sacroiliacum anterius - Fifth lumbar vertebra -
Vertebra lumbalis V - Fourth lumbar vertebra -
Vertebra lumbalis IV - Tailbone -
Coccyx - Pubic bone -
Pubis - Thigh shaft -
Corpus femoris - Lumbar cruciate ligament kink -
Promontory
You can find an overview of all Dr-Gumpert images at: medical illustrations
Gender-specific differences in the articular surfaces
In women, the joint surface is much more even, so that there is much greater freedom of movement than in the ISG of the man exists.
The stabilizing factors of the joint in women are on the one hand the position of the sacrum in the pelvic ring and on the other hand the muscles and ligaments. One speaks of the so-called Frictional connection of the joint.
The surfaces of the joint surfaces in men are characterized by numerous grooves and elevations, so that a lot of force has to be used to achieve a displacement of the joint surfaces against each other. The result is great stability but little mobility of the joint. One speaks of the so-called Form fit of the joint.
Stabilizing factors of the ISG
In addition to the surface quality of the joint surfaces and the position of the sacrum in the Pelvic ring A number of ligaments are responsible for the stability of the SI joint.
The most important bands are briefly described below.
- Posterior sacroiliac ligament (ligg.sacroiliaca dorsalia)
These are fiber strands that connect the iliac bone with the Sacrum connect. - Anterior sacroiliac ligaments (ligg.sacroiliaca ventralia)
These ligament structures also connect the iliac bone with the sacrum, are rather thin and have a connection with the capsule. In their upper fiber course they form a connection with the ilio-lumbar ligament. - Ligg. sacroiliaca interossea
These ligaments, the fiber strands of which are very dense and short, also connect with the joint capsule and fill the sacral sulcus. Due to their direct positional relationship to the capsule and by filling the sacral sulcus, they play an important role in stabilizing the SI joint. - Ligg. sacrospinale
This ligament has its origin on the lower outer surface of the sacrum and the base of the coccyx, runs in front of the sacrotuberous ligament, with which it is closely connected, and starts in the area of the sciatic spine. - Sacrotuberous ligament
This triangular ligament arises on the side areas of the sacrum / coccyx and iliac bone (spina iliaca posterior superior (SIP)) and starts at the ischial tuberosity.
This ligament also plays an important role in stabilizing and moving the ISG. Together with the sacrospinal ligament, it is the strongest ligament for stabilizing the nutation movement.
The sacrospinal ligament and the sacrotuberous ligament
make a major and minor sciatic notch Foramen isciadicum major and minor. These are important passageways for vessels, annoy and Muscles represent. - Iliolumbar ligament
They continue the posterior sacroiliac ligaments upwards and pull from the iliac bone to the 4th and 5th Lumbar vertebrae . These ligaments are responsible for stabilizing the anterior SI joint area.
Appointment with a back specialist?

I would be happy to advise you!
Who am I?
My name is I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me live every 6 weeks on "Hallo Hessen".
But now enough is indicated ;-)
The spine is difficult to treat. On the one hand it is exposed to high mechanical loads, on the other hand it has great mobility.
The treatment of the spine (e.g. herniated disc, facet syndrome, foramen stenosis, etc.) therefore requires a lot of experience.
I focus on a wide variety of diseases of the spine.
The aim of all treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- - your orthopedic surgeon
14
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
You can find more information about me at
Function of the ligaments as a whole
The ligaments described are the most important structures for stabilizing the SI joint and preventing unphysiological movements in this joint.
If there are malfunctions in the SI joint with incorrect posture or malpositions of the intestinal or sacrum, the affected ligaments are put under increased strain.
Provocation tests for the ligaments
The ligaments are tested and provoked in the supine position. Here you bend the patient's leg and stretch the ligaments in different positions of the Hip joint exerts a thrust along the longitudinal axis of the thigh.
- To test the iliolumbar ligament, guide the knee towards the opposite hip joint
- To test the sacrotuberous ligament, bring the knee to the shoulder on the same side
- To test the Ligg. sacroiliaca dorsalia and sacrospinale, the knee is brought to the opposite shoulder.
As a practical tip, it has proven to be beneficial that the Stretching of the ligaments hold it for a while and feel it (palpate).
Innervation of the SI joint (nerve supply)
The sacroiliac joint is mainly supplied from the nerve root S1 (nerve from the sacrum). The Ligg are an exception. sacrotuberals and sarospinals that are supplied from segments S3-4.
Axes of motion

In the ISG, movements take place around different axes of movement, the intersection of which is at the level of the second sacral vertebra.
- Frontal axis
The flexion and extension movements (bending and stretching) of the SI joint take place around this axis. It is an imaginary line that runs horizontally through the second sacral vertebra.
The flexion and extension movements are also known as nutation and counter-nutation. - Longitudinal axes
The sacrum rotates around this axis when walking and thus allows slight rotational movements.
It is a vertical line that divides the sacrum into right and left halves. - Diagonal axes
These are two axes that run diagonally through the sacrum. The right one runs from the upper right to the lower left pole, the left one from the upper left to the lower right pole.
Since the torsional movements take place around these axes when walking, they are also referred to as torsion axes. - Sagittal axis
It is the intersection of most of the axes and runs from the front and back through the second sacral vertebra.
The sagittal axis is very important for the balance of the sacrum.
Range of motion
The degree of mobility is very low. Active movement is not possible.
Movements while walking
During the Walking there are minimal but changing movements in the SIGs. The movements in the ISG should be made clear by the step with the right leg.
- At one step with that right leg the right ilium (iliac bone) moves backwards. The ilium rotates around the longitudinal axis to the left, while the left one moves forward. An additional torsional movement (turning movement) around the left torsion axis causes the sacrum base to tilt to the left.
- From the transition to the middle standing leg phase, the right coxae rotates forwards and the left one backwards. As a result, it turns Sacrum to the right and its base descends on this side.
Practical tip
Testing of joint play and muscles
In the case of malfunctions in the ISG, it is important whether the cause is a malfunction of the Joint play or the Musculature lies.
Usually both disorders are coupled to each other. Various tests are carried out to examine the joint play. For general understanding, one joint partner is fixed and the other is moved (mobilized). If there is a side difference, it is a matter of reduced joint play on the poorly sliding side. In addition, the associated muscles must be checked for their ability to stretch.
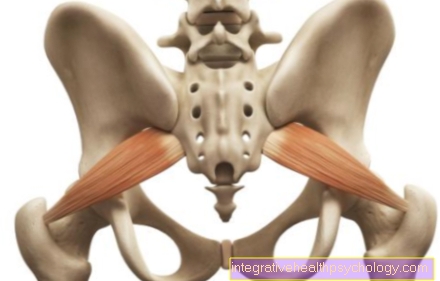
Muscle training for SIG instability
In the case of joint instability, the SI joint should not be mobilized or manipulated, but the corresponding muscles should be trained for stabilization. Of particular importance are the M.erector spinae and the M. piriformis.
Since muscle building usually involves ongoing movement in the ISG, an attempt must be made to prevent this. It is therefore important to first passively stabilize the pelvic ring and only then to train the muscles.
ISG blockage / ISG blockage

A sacroiliac joint blockage refers to reduced mobility of the sacroiliac joint. SI joint blockade, SI joint blockage (sometimes the joint is also abbreviated as SIG) and hypomobility of the sacroiliac joint are used synonymously. Physiologically, the SI joint has very little mobility and cannot be moved consciously. This joint is held in place by tight ligaments.
Changes in the joint surface (e.g. due to wear and tear or diseases associated with inflammation of the SI joint) and the surrounding soft tissues including the ligaments can lead to a blockage of the joint. Often it comes to sudden onset pain in the area of the lower back (lower lumbar vertebrae) and the buttocks. The pain is movement-dependent and can be aggravated by some movements. Some people wake up from pain at night and need to lie down in a different position to relieve the pain. The nature of the pain can range from short-term, stabbing pain to constant dull pain.
Reasons for a blockage of the ISG can be heavy lifting, excessive strain in sports, overstretching of the ligaments or unusual movements such as an unwanted "step into the void" when stumbling on the stairs. Monotonous work or unfavorable postures can also lead to an ISG blockage.
Some conditions affecting the spine are associated with a higher risk of blockage of the SIJ.These can be diseases that lead to improper stress on the hip or those that directly affect the sacroiliac joint, such as ankylosing spondylitis, which is very often associated with inflammation of the sacroiliac joint. Inflammatory bowel diseases (Crohn's disease, ulcerative colitis) also suffer from inflammation in the sacroiliac joint in some of those affected.
Diagnostically, the so-called pseudoradicular complaints with an ISG blockage must be differentiated from the radicular pattern with herniated discs of the lower lumbar spine. (In a herniated disc, the nerve roots are squeezed as they exit the spinal canal.)
In the case of a herniated disc of the lumbar spine, the SI joint is often blocked. Therefore, if there is a herniated disc of the lumbar spine and an ISG blockage at the same time, the question arises about the hen and the egg!
First of all, the exact course of the pain is used as a distinguishing feature. In the case of a herniated disc, these run along a dermatome, that is, along the supply line to the affected nerve root. The pain from an SI joint blockage does not adhere to these limits. In addition, the reflexes are not weakened and there is no muscle weakness on the affected side.
From a therapeutic point of view, pain medication is initially useful to reduce pain symptoms. So-called non-steroidal anti-inflammatory drugs such as ibuprofen or diclofenac are used for this. Muscle relaxants can also help to counteract the pain-related tension. Local heat can also help relax muscles. Movement should not be avoided in general. There are some exercises that can help release the blockage by moving the sacroiliac joint. It can happen that you hear a "cracking" sound while moving and the pain subsides a little. The exercise should then not be interrupted, but repeated a few more times. Different exercises can be done alone (see exercises). There are also some handles that a therapist (e.g. a physiotherapist) can use to release an ISG blockage. Usually this will reduce the pain, but it may take a few days for it to go away completely.
Read more about these topics at:
- ISG blockage
- ISG blocking
Figure ISG - blockage

ISG - blockage - conduction symptoms
- Sacrum-iliac joint
(Sacroiliac joint,
abbreviated ISG)
Articulatio sacroiliaca - Front Sacrum-iliac ligament
Lig. Sacroiliacum anterius - Iliac bone - Os ilium
- Sacrum - Sacrum
- Lumbar and sacrum kink -
Promontory - Fifth lumbar vertebra -
Vertebra lumbalis V - First lumbar vertebra -
Vertebra lumbalis I - Thoracolumbar junction
- Twelfth thoracic vertebra -
Vertebra thoracica XII - Hip joint - Articulatio coxae
Pain radiation areas:
A - lumbar spine (lumbar spine)
B - buttock region - Gluteal region
C - Groin - Inguinal region
D - leg front and back
E - knee
You can find an overview of all Dr-Gumpert images at: medical illustrations
Inflammation of the SI joint / sacroiliitis
An inflammation in the sacroiliac joint is called sacroiliitis in medical parlance. The inflammation in the sacroiliac joint (sacroiliitis) can lead to destruction of the joint with severe pain and the possible consequence of irreversible postural damage. In the last stage of the disease, there is complete osseous stiffening of the joint (so-called ankylosis). An inflammation of the SI joint can be proven by various imaging methods. Magnetic resonance imaging (MRI) is the method that detects changes in the very early stages. More advanced stages can also be seen in classic X-rays and in computed tomography (CT) examinations.
Inflammation of the sacroiliac joint (sacroiliitis) is usually not found as an isolated disease, but as a symptom of an underlying disease.
Typical underlying diseases associated with sacroiliitis are:
- ankylosing spondylitis
- Behçet's disease
- Reactive arthritis
and - especially Reiter's disease
- Psoriatic arthritis
and - inflammatory bowel disease such as Crohn's disease
and - ulcerative colitis.
Bechterew's disease is a rheumatic disease. More men are affected. In addition to inflammation in the sacroiliac joint (sacroiliitis), changes in the spine often occur with increasing stiffening. In addition, inflammation of various joints and the insertion tendons of muscles (for example the Achilles tendon) are typical.
Behcet's disease is particularly common in the Mediterranean region and, in addition to inflammation of the SI joint (sacroiliitis), often has canker sores in the mouth and genital area, various skin rashes, inflammation in joints and eye diseases as symptoms.
You can find out more about this disease at: Behçet's disease
Reactive arthritis is inflammation of the joints that occurs a few days after the upper respiratory tract becomes infected with the bacterium Streptococcus.
Reiter's syndrome describes the simultaneous occurrence of conjunctivitis, joint inflammation and inflammation of the urinary tract.
Psoriatic arthritis is a special form of psoriasis that is associated with joint inflammation.
In general, the treatment of the underlying disease is in the foreground. Cortisone or other immunosuppressants (such as methotrexate (MTX)) are often used.
Read more on this topic at: Sacroiliitis
ISG syndrome
The ISG syndrome is not uniformly defined. It includes various diseases associated with sacroiliac joint pain. It can therefore be used as a Collective term can be seen, which includes various diseases of the sacroiliac joint. Sometimes the term sacroiliac joint syndrome refers to diseases that lead to chronic complaints. Typical pains are included Back pain, especially in the pelvic area (also Lower back pain). There is also pain in the area of the Buttocks and lateral pelvis and in the Groin area in front.
Typical causes of an ISG syndrome are arthrosis as a sign of wear and tear, overstressing and overstressing the ligament apparatus, inflammation in other underlying diseases (e.g. ankylosing spondylitis) and by loosening the ligamentous apparatus in women in the pregnancy and after childbirth.
During pregnancy, loosening of the ligamentous apparatus is a desired and necessary process, as it makes the birth process possible through a somewhat greater mobility within the sacroiliac joint.
Various clinical tests can be carried out as diagnostics if an ISG syndrome is suspected. That is typical Forward phenomenon, in which the examiner on both sides of the standing patient Bony prominence of the pelvis (so-called Spinae iliacae posteriores superiores: these can be felt on the back by following the iliac blades from above towards the buttocks). At these points there is also a typical one Tenderness in ISG syndrome. When the patient slowly bends over, an assessment is made of whether these protruding bones are moving forward evenly on both sides. If this is not the case, this indicates a blockage within the sacroiliac joints. There are a few other clinical tests that induce movement within the sacroiliac joint and the painfulness of these tests suggests SI joint syndrome. The diagnosis can be made in conjunction with typical triggers, such as one-sided posture when sitting or exercising.
Imaging procedures such as roentgen-, CT- or MRI- Examinations are usually not necessary. In individual cases, however, they can be useful if the course of the disease is complicated or if chronic inflammation of the SI joint (sacroiliitis) is the cause of the symptoms.
Therapeutically, the ISG syndrome comes first conservative Measures under consideration. This includes combating pain with classic Painkillers (for example Ibuprofen). Physiotherapeutic measures and avoidance of special stressful situations can also help. In severe cases (possibly also CT-controlled) an injection of the painful Joint With Local anesthetics and cortisone-like substances are offered. One is also very rare operational Therapy with stiffening of the ISG considered.
Arthrosis of the SI joint
A arthrosis in the sacroiliac joint arises from the heavy load on this joint over years. The sacroiliac joint (also known as the sacrum-iliac joint) connects the spine with the pelvis and is therefore a central point of transmission of the force from the back, head and arms to the pool and the legs. Due to the upright gait, very strong forces are transmitted here. In order to deal with these forces, the joint is secured by very strong and tight ligaments and allows only minimal movements.
The tapes are going through now heavy loads For example, if you are stressed by heavy physical work for years and there is a little more mobility in the joint, rubbing the joint surfaces can lead to osteoarthritis. There the joint surfaces wear out, the Cartilage becomes thinner, the surface is no longer smooth but rough. With every movement, the rubbing of these rough surfaces creates painful stimuli. In the case of high stress situations, a locally limited inflammation arise, which intensifies the pain (so-called activated osteoarthritis).
Typical symptoms of sacroiliac joint arthrosis are deep back pain, Pain in the buttocks and partially Radiation of pain into the leg. Also Paresthesia in the affected skin area are possible. The symptoms are similar to and can be confused with irritation of the sciatic nerve.
Sacroiliac joint arthrosis is diagnosed by the typical symptoms and a corresponding history. Many too Births can be a risk factor for SI joint osteoarthritis due to the loosening of the ligamentous system. In addition, a clinical examination is carried out by an experienced examiner. The diagnosis can be supplemented by x-rays.
In the early stages, treatment of pain and controlled movements under physiotherapeutic guidance come into play. Also other conservative treatments like Osteopathy, Stimulation current and acupuncture can help. So-called local infiltration can be used for severe pain. In doing so, (possibly under imaging control by means of CT or roentgenFluoroscopy) on and into the joint Local anesthetic often together with one cortisone-like drug injected. In this way, relief can be achieved, especially in phases with particular pain peaks.
As last chance becomes a surgery viewed. This is where the joint Stiffened with screwswhich prevents further rubbing of the two articular surfaces against each other, but to one Loss of function leads.
Exercises
There are a variety of exercises that can help with sacroiliac joint blockage. These should be explained in detail by a physiotherapist or orthopedic surgeon and applied after a thorough examination. These exercises help to move the sacroiliac joint and thus to release blockages.
A simple exercise that can be done at home is a pendulum swing in the pelvis. To do this, stand on an elevation (e.g. a thick book) and swing the other leg slightly back and forth. If you move the pelvis of the supporting leg a little forward with one hand while swinging back, you can increase the movement in the ISG. If you have balance problems, you should do this exercise on a wall where you can support yourself with both hands.
Another exercise in the supine position is, for example, careful cycling. The legs are bent at right angles in the knee joint and hip joint and one makes careful circular movements with the legs as when riding a bicycle. In the supine position, you can also put both hands under the sacrum and then slowly circle the pelvis in all directions.
In the 4-foot stand (kneel supported on knees and hands) the legs are alternately stretched out so that they form a straight line with the back. You can also do the exercise from time to time as a precaution, while at the same time stretching the other arm (i.e. diagonally left leg, right arm) forward.
As a prophylactic measure, you should avoid unfavorable sitting positions, heavy lifting and carrying, and jerky movements in the hip joint. In general, light sporting activity is beneficial to strengthen muscles and tendons and to prevent an ISG blockage.