AO classification
Definition / introduction
The AO classification (=Working group for osteosynthesis issues), also called the Müller classification, was introduced in order to be able to provide a clear description of fractures. This classification is valid worldwide and serves as the basis for standardized bone fracture treatment. It is possible to describe fractures in a standardized way and thus to treat them in a standardized way.

history
The Working group for osteosynthesis issues (AO classification) was founded in 1958 by 13 surgeons and orthopedists. The management of the training community took over Maurice E. Muller, Martin Allgöwer, Robert Schneider and Hans Willenegger. The headquarters of the AO are in Davos (Switzerland). 1984 the working group was reorganized in the form of a non-profit foundation. Today the working group for osteosynthesis questions has about 5000 members and has become an important network between surgeons. The AO has set itself the task of promoting and standardizing medical progress in operative bone fracture treatments for diseases of the musculoskeletal system. Because of this, the AO classification introduced to describe bone fractures.
Structure of the AO classification
The AO classification consists of a 5-digit alphanumeric code. This describes the exact location and severity of the fracture. If, in addition to the bone fracture, there is also soft tissue damage, skin or vascular damage, further codes are used. Special codes are also used for broken feet and hands, as well as breaks in childhood. The AO classification is mainly used in the context of fractures of the long tubular bones (e.g. thigh bones).
In order to be able to use the AO classification in a standardized way, different numbers are assigned to the body regions and injury patterns:
The most common use is the AO classification on the upper arm (humerus) = 1, forearm (radius = spoke, ulna = ulna) = 2, thigh (femur) = 3 and lower leg (tibia = shin, fibula = fibula) = 4. The Body region comes first in the code. All other bones in the body are also numbered and can thus be described with the AO classification. However, this is mainly used for the bones mentioned above, which is why only these are specifically listed here.
The fracture must be precisely localized within a body region. A distinction is made between the bone end near the body (= proximal) = 1, the Bone shaft (diaphyseal) = 2 and dem Far end (= distal) = 3. The inner and outer knuckles (malleoli) form an exception and are coded with the number 4. The location is the second in the code.
In addition, the fractures must be classified according to their severity, prognosis and the degree of difficulty of their treatment. Shaft fractures are divided into three groups: A = simple fracture, B = wedge fracture, C = complex fracture. If the fracture affects the joint, this fracture is also divided into 3 groups: A = outside the joint space (extra-articular), B = partial (partial) joint fracture, C = complete joint fracture. The severity of the fracture is indicated in the third position of the code. In addition, the severity of the break is generally coded as easy = 1, medium = 2 or difficult = 3.
Appointment with ?

I would be happy to advise you!
Who am I?
My name is I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
In order to be able to treat successfully in orthopedics, a thorough examination, diagnosis and a medical history are required.
In our very economic world in particular, there is too little time to thoroughly grasp the complex diseases of orthopedics and thus initiate targeted treatment.
I don't want to join the ranks of "quick knife pullers".
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You will find me:
- - orthopedic surgeons
14
You can make an appointment here.
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
For more information about myself, see - Orthopedists.
example
To clarify and better understand the AO classification, the following 2 examples are given:
32- A1: This would be the code for a thigh fracture (3) concerning the bone shaft (2). It is a simple fracture (A) that is generally classified as a mild fracture (1).
21- C3: This code stands for a forearm fracture (2) that affects the end of the bone near the body (1). It is a complex fracture (C) that is classified as a severe (3) fracture overall.
AO classification on the radius (spoke)
The AO classification on the radius (spoke) is used to classify broken bones in the forearm in the area of the wrist. A distinction is made between three groups of bone fractures, which in turn can be divided into subgroups. The decisive factor for the classification is whether there is an injury to a joint. If only a broken bone of the spoke (radius) or cubit (Ulna) is present without joint involvement (extra-articular fracture), it is a type A injury according to the AO classification. In A1 only the ulna is affected and in A2 the spoke is single, in A3 it is broken several times.
In group B injuries are classified in which the joint is partially affected (partial joint fractures). Here, too, a distinction is made between injury types B1, B2 and B3, depending on which joints are involved. The most severe are the radius fractures of type C according to the AO classification. They are complete joint fractures. Depending on which and how many bones are broken, a distinction is also made here into the subtypes C1, C2 and C3.
Read more on the topic: Broken spoke / radius fracture
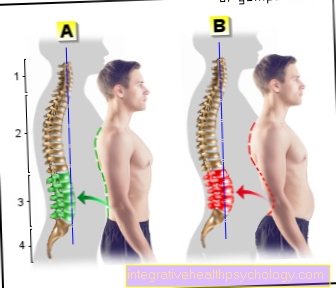
AO classification on the spine
On the spine, fractures of the vertebral bodies (Vertebral body fractures) based on the AO classification. The classification is particularly important as it enables a distinction to be made between stable and unstable injuries to the spine. A stable fracture can be treated conservatively (that is, without surgery). An unstable fracture, on the other hand, must be stabilized by surgical intervention. The injuries are divided into types A, B and C.
Type A is also called a compression injury.The force that causes the fracture comes from above (often, for example, a fatigue fracture in older women with bone loss). Type A injuries are mostly stable because the back of the vertebral body is intact.
Vertebral body fractures of type B and type C, on the other hand, are unstable, since the rear part of the vertebral body is also affected by the injury. Such injuries can occur, for example, in a serious traffic accident. Type C differs from type B mainly in the nature of the injury. In type C, rotational forces also lead to the injury, while this is not the case with type B. In both cases, however, an operation usually has to be carried out promptly in order to prevent an injury to the spinal cord and any associated paralysis.
Read more on the topic: Vertebral fracture