Endocarditis
Synoyme in the broader sense
Heart valve inflammation, heart wall inflammation
introduction
Inflammation of the heart valves (endocarditis) is a potentially life-threatening disease, usually caused by microbial pathogens such as viruses, bacteria or fungi.Structural damage to the heart valves associated with a functional defect is not uncommon as a result.

Symptoms of Endocarditis
The symptoms of endocarditis are often flu-like in the beginning and indistinguishable from other general diseases, which makes a clear diagnosis difficult.
Stand in the foreground
- Fever, initially around 38 ° C
- easy physical fatigue
- Loss of appetite
- A headache.
Weight loss, chills, sweats, muscle and joint pain can also occur.
After a prolonged course of the disease, a pale skin color, which is due to anemia and a general feeling of weakness, can be observed.
With existing, hemodynamically relevant (i.e. affecting the blood flow) valve damage, shortness of breath is the main symptom of endocarditis: If a heart valve no longer closes properly (= Valve insufficiency), during the phase of the filling of the heart chambers (the phase of the heart's actions is called diastole) blood flows back into the atrium and this wears out (medical: he dilates). The returning blood is also responsible for the fact that larger amounts of blood than normal have to be pumped from the heart into the body. As a result, the heart enlarges (hypertrophy); comparable to a heavily trained muscle. This naturally occurring process of adaptation of the heart muscle to overtime becomes harmful if it becomes so large that the supplying blood vessels can no longer guarantee an adequate supply of oxygen.
In men this is the case when the so-called critical heart weight of 500g is exceeded, in women it is 400g.
In the context of endocarditis, not only leaks in the valves, but also narrowing (so-called stenoses) of the outflow path can be the result.
As with valve insufficiency, when the heart valve is narrowed (stenosis), while the heart muscle contracts in the so-called ejection phase (systole), insufficient oxygen-rich blood enters the internal organs and the person concerned also suffers from shortness of breath (medical: Dyspnea).
One way to diagnose endocarditis is what is known as a swallow echo. This involves testing the functioning of the heart by swallowing an ultrasound head.
Read a lot more information under our topic: Symptoms of endocarditis
therapy
Treatment is with antibiotics, as it is often triggered by bacterial pathogens. It is important to start therapy early to avoid complications of the infection. Different antibiotics are used depending on whether the affected heart valve is the patient's own original heart valve or a valve prosthesis.
In the case of endocarditis of the native valves - the patient's own heart valves - the antibiotics ampicillin-sulbactam, amoxicillin-clavulanic acid, ciprofloxacin and gentamicin are used. The same active ingredients are used to treat a valve prosthesis after the first year after the operation. The duration of therapy in this case is usually four to six weeks.
If the valve operation is less than a year ago and the corresponding heart valve is then affected by endocarditis, the antibiotics vancomycin, rifampicin and gentamicin are preferred. Vancomycin and rifampicin are usually administered for six weeks or more, gentamicin for around two weeks. The treatment of endocarditis must be intravenous, which means that the antibiotics are given directly into a vein by infusion. Only in this way does enough of the active ingredient reach the heart valves so that the bacteria can be killed. This is due to the fact that the heart valves themselves are not supplied with blood and the drugs therefore only reach their target site through the bloodstream through the heart cavities.
Accordingly, patients with endocarditis are treated in the hospital. The success of the therapy must be checked regularly. If the heart valve is severely affected, surgical repair may need to be considered to avoid complications. Otherwise, parts of the growths on the heart valve can loosen and cause strokes, for example. Even if there is a risk of heart failure or other complications, surgical therapy is often necessary.
Read more on the subject at: Therapy of endocarditis
Endocarditis Guideline
The guideline on endocarditis is regularly revised and adapted to the latest medical knowledge. The guideline contains recommendations for action for doctors treating patients with the corresponding disease and accordingly shows the most tried and tested diagnostic and therapeutic measures. The doctors are not bound by the guidelines, but can only use them as a guide. The guideline also gives recommendations for endocarditis prophylaxis and important hygienic measures that must be observed in contact with patients suffering from endocarditis.
The use of the guidelines is intended to generally improve the standardized care of patients with various diseases by providing all doctors with comprehensive recommendations for diagnostics and therapy that correspond to the latest doctrinal opinions.
forecast
About thirty percent of all those affected respond poorly to the medication (antibiotics), so that it becomes far-reaching Damage to the heart valves comes.
Then an operation with replacement by artificial valves is often inevitable as a life-saving measure.
Complications
Dreaded complications of heart valve inflammation (Endocarditis) represent settlements of bacterial deposits on the heart valves. These are called vegetation and can be thought of as small clusters of bacteria that grow on the heart valve.
These can be carried away by the pumping heart with the bloodstream and then the blood supply to other internal organs by closing the supplying vessel through the "Clusters of bacteria”Interrupt.
The consequence of these so-called septic embolisms are functional failures of the corresponding organ with the respective characteristic complaints.
Is this brain affected, threatens a life-threatening heart attack (Stroke = apoplexy).
When the lung supplying vessels (rarely is the pulmonary artery itself blocked by a clot because it is the largest in diameter) it comes to itself primarily through severe shortness of breath, accelerated breathing (Tachypnea), chest pain (Chest pain), as well as in extreme cases through unconsciousness Pulmonary embolism (see below).
Will the kidney If the vessel supplying it is no longer adequately supplied with blood, the filtration of the blood through the small blood capillary loops of the kidneys (the so-called glomeruli), which serve as filters, is no longer possible and urine production ceases:
Levels of Kidney failure:
- Oliguria: with less than 500 ml, too little urine is produced in 24 hours
- Anuria: no urine or less than 100 ml urine is produced in 24 hours
As with all organs, the extent of functional failures and complaints depends on the size of the closed vessel.
Small kidney infarcts often go unnoticed, while larger ones with sudden flank pain, Vomit, nausea and fever accompanied. Due to the kidney damage, blood and proteins can be detected in the urine.
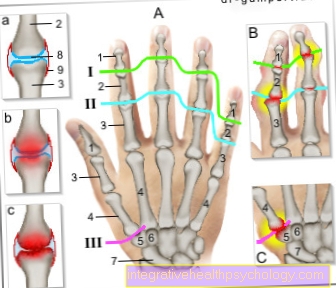
Small clots also lead to punctiform bleeding skin (so-called. Petechiae) and are often important guides in recognizing the Myocarditis (Endocarditis).
Typically, they appear on the fingertips and feet. According to their first description, the internist Sir William Osler (in 1885), the 2 to 5 mm large, non-painful skin changes are considered to be Osler nodules designated. This disease is not to be confused with the Osler's disease.
Inflammation of the heart muscle (endocarditis) itself has long been known and was found in 600 to 700 year old mummies in South America.
Duration of endocarditis
The endocarditis should treated early in order to avoid complications and consequential damage. If the antibiotic therapy is started in time, the disease will sound like over the duration of the therapy about four to six weeks off again. That is important regular control of the therapy success, since this is the only way to ensure that complications have not occurred.
Since the heart valves are not supplied with blood, it is for the body alone extremely difficult to fight the infection without therapy. That is why the timely medical care of affected patients is so important and enables the disease to be limited to a period of a few weeks.
Forms of endocarditis
Acute endocarditis
Acute endocarditis, as the name suggests, represents the highly acute form of the disease. It is in contrast to lenta endocarditis, which only progresses slowly and can be accompanied by little or no symptoms.
In acute endocarditis, however, the symptoms, changes and life-threatening complications often occur within a few hours. Initially, there is also a fever, weakness and an increased heart rate. However, heart murmurs, a racing heart, heart valve damage and even heart failure can quickly follow. In this special case, antibiotic therapy must be initiated as soon as possible, as so-called "staphylococci" are mainly responsible for this form of endocarditis.
Surgical intervention may also be necessary in the event of severe complications. Here destroyed valves are reconstructed and all potentially infectious components are removed, if possible.
Endocarditis lenta
Endocarditis lenta is a subtype of general endocarditis and contrasts with acute endocarditis as a further form. While the latter manifests itself in a very sudden, acute and often severe course, endocarditis lenta is a gradual form. Most often it is caused by the pathogen Streptococcus viridans. Within weeks to months, the pathogen forms its settlements and growths on the heart valve and gradually leads to the typical symptoms. However, due to the comparatively slow process, these can often initially be misunderstood and only become noticeable subliminally. In the course of the disease, there is often fever and fatigue, loss of appetite and anemia. As the disease progresses, the general condition of the patient continues to deteriorate, so that the symptoms become more pronounced at some point.
Libmann-Sacks endocarditis
Libmann-Sacks endocarditis is a variant of the disease that has no infectious cause and can therefore be described as sterile. Neither bacteria nor other pathogens cause the changes in the inner walls of the heart, rather autoimmune diseases are probably behind the endocarditis. The autoimmune disease lupus erythematosus is often the underlying cause. Autoimmunological processes in the body cause deposits of various cells in the blood to form on the heart valves.
As a result, crusts form on the heart valves, which are often harmless, but in rare cases can lead to discomfort and harmful changes to the valves. Sometimes the cords of the heart can tear and valve insufficiencies can develop.
Often, however, Libmann-Sacks endocarditis remains symptom-free and undetected.
Rheumatic endocarditis
Rheumatic endocarditis is a complication of rheumatic fever, an autoimmune disease associated with a bacterial infection.
In most cases, there was a streptococcal infection in the throat about two weeks before the symptoms. The infection itself can be harmless, but as a result the body can develop antibodies against the body's own structures, which can lead to fever, weakness, fatigue and rheumatic changes in the joints.
One of the dreaded complications of rheumatic fever is the involvement of the heart in the form of rheumatic endocarditis. Here, cells of the blood attach to the heart valves and can cause scars and calcifications.
As a result, changes in the heart valves can occur, which can have serious consequences. In the treatment of severe cardiac involvement, the immune system must be suppressed with drugs to control the body's own antibodies.
Is Endocarditis Contagious?
Endocarditis is usually not contagious. It is only triggered by small amounts of bacteria, which are found in many places in the mouth or in the body and can only get into the bloodstream through minor injuries.
The infectious focus is then only on the heart, where small abscesses, encapsulations of the bacteria can form.
Disease origin and cause
The prerequisite for an inflammation that leads to structural damage to the heart valves is an increased flushing of pathogens into the blood (this is also known as bacteremia).
Frequent starting points ("foci" of the endocarditis) are:
- purulent skin inflammation (so-called boils = large pimples)
- Ear, nose and throat infections (such as:
- purulent tonsillitis, medical: tonsillitis
- Inflammation of the paranasal sinuses = inflammation of the paranasal sinuses, medical: sinusitis
- Inflammation of the lungs (pneumonia)
- Dental infections
- Bacteremia
In healthy people, the increased bacterial load leads to an activation of the immune system: white blood cells produce the body's own proteins (so-called antibodies) in order to mark the pathogens as foreign invaders, so that they can then be removed from phagocytes (which represent a separate subgroup of white blood cells and also called macrophages) are eliminated.
In the case of previous damage (see above), depending on the aggressiveness of the pathogen and the immune system of the person concerned, valve destruction is rapid (acute is a disease progression within 40 days).
The so-called subacute endocarditis proceeds insidiously; the complaints (see below) are much less pronounced here than in the acute form. The reason is that numerically different, less aggressive pathogens are decisive.
Another form of the inflammation of the inner wall of the heart, which has become rare today due to antibiotic prevention, is a hypersensitivity reaction of our immune system.
In contrast to the form primarily caused by pathogens (and therefore also referred to as "infectious endocarditis"), the inflammation takes place inside the valve.
Responsible is a preceding inflammation caused by so-called beta-hemolytic streptococci, when attempting to control it, the body's own antibodies react not only with the wall components of the pathogen, but also with the body's own components of protein molecules of the heart or joints that happen to look similar.
While the term “rheumatic fever” describes the reaction of the entire body, the subcomponent that specifically affects the heart is referred to as “endocarditis rheumatica”.
Rarer special forms of the heart inflammation occur in:
- Cancer diseases ("endocarditis marantica")
- Autoimmune disease lupus erythematosus ("endocarditis thrombotica Libman-Sacks")
An allergic trigger is suspected in the "endocarditis parietalis fibroplastica Löffler" leading to heart failure / heart failure due to excessive connective tissue formation.
Pathogen
Usually are different bacteria the causative agents of infectious endocarditis. Most often it is Staphylococci, especially the bacterium Staphylococcus aureus. This is for about 45-65% responsible for endocarditis. The second most common endocarditis pathogen is one of the Streptococci and is referred to as Streptococcus viridans. He caused about 30% of endocarditis.
Other pathogens that come into question but occur significantly less often than those already mentioned are, for example, Staphylococcus epidermidis, Enterococci, more streptococci as well Mushrooms (Aspergillus fumigatus). The latter mainly play a role immunocompromised patients play a role, for example, in patients with HIV, after organ transplants or chemotherapy.
How does the diagnosis of endocarditis work?
The diagnosis differs according to whether there is a suspicion of infectious bacterial endocarditis or non-pathogen-related endocarditis. Infectious endocarditis is diagnosed using several criteria.
The two most important criteria are so-called "positive blood cultures" and abnormalities in the ultrasound or CT examination. In order to obtain the former, blood is drawn from the patient at several points. This is injected into special bottles in which bacteria can be grown. The so-called “blood cultures” are used to detect bacteria that circulate in the blood and provide an important indication of possible endocarditis.
If the ultrasound examination also reveals abnormalities in the inner walls of the heart or valves, the suspicion of endocarditis is confirmed. If these main criteria are not adequately met, further examinations can be used in order to be able to make the diagnosis of endocarditis anyway.
Other important criteria that can corroborate a suspected diagnosis are drug abuse, other heart diseases, high fever or certain vascular diseases.
Illustration heart with heart valves

- artery (aorta)
- left atrium
- left atrial valve = mitral valve (closed)
- left heart valve = aortic valve (open)
- left ventricle
- right ventricle
- inferior vena cava (inferior vena cava)
- right heart valve = pulmonary valve (open)
- right atrium
- superior vena cava (vena cava superior)
Endocarditis prophylaxis
The recommendations for endocarditis prophylaxis have been increasingly limited in recent years in order to avoid unnecessary antibiotic administration and thus to prevent the increasing resistance of bacteria. Endocarditis prophylaxis is recommended nowadays for patients with heart valve replacement, patients with endocarditis, patients with certain congenital heart defects, or operated heart defects with the use of prosthetic material.
Since there is no general agreement as to the extent to which endocarditis prophylaxis should also take place, it is ultimately a matter of individual decision-making. Prophylaxis includes the administration of antibiotics and should be carried out in particular after surgery in the mouth and throat, for example in the case of dental treatments such as the removal of tartar and root canal treatments, in the removal of the tonsils (Tonsillectomy) and other interventions in this area. In high-risk groups, endocarditis prophylaxis is also recommended for many other surgical interventions, for example interventions in the gastrointestinal or respiratory tract, as well as in the urogenital tract.
The antibiotic is administered about 30-60 minutes before the procedure. For dental interventions, amoxicillin or ampicillin are preferred; for interventions in the urogenital or gastrointestinal tract, ampicillin or piperacillin are used. The selected antibiotics are based on the expected bacterial flora of the operated area. In the case of special germs, the antibiotic prophylaxis must be adapted accordingly.
Find out more about the topic here: Endocarditis prophylaxis
Frequency (epidemiology)
In the Federal Republic of Germany there are around 2 to 6 new cases of endocarditis per year among 100,000 inhabitants.
Men are affected twice as often as women on average. The peak of the age of endocarditis is 50 years.
Since the introduction of antibiotic therapy, the incidence of the disease has not decreased overall (which would have to be assumed due to the improved therapy), however, the heart valve inflammation occurs around 15 years later than before and other germs are responsible as triggering factors.
Various factors lead to a significant increase in the risk of the disease:
- Congenital heart valve defects (mostly the valves of the larger left ventricle are affected, i.e. the aortic valve and the mitral valve separating the atrium and ventricle)
- congenital malformations of the heart
- Heart surgery
Bacteria circulating in the blood make it easier for them to adhere to the sensitive inner wall of the heart, which is medically called the endocardium. This skin, made up of connective tissue, smooth muscle cells and elastic fibers, also covers the heart valves.
This explains why people with healthy hearts are less likely to develop heart valve inflammation (endocarditis). In the first year after a heart valve (artificial heart valve) has been replaced, around 2 to 3% of those who have been operated on develop heart valve inflammation. In the following years, the risk decreases again.
Furthermore, all processes associated with a weakening of the body's immune system represent an increased risk. on the one hand diseases of the blood-forming system (white blood cells, so-called leukocytes, perform the important task of defending our body against specific intruders), diabetes mellitus (= diabetes; see diseases of the pancreas) or chemotherapy.
Drug addiction promotes the occurrence of heart valve inflammation (endocarditis), as intravenous injections often lead to the spread of germs, which then reach the right heart directly via the superior vena cava and mainly damage the valve separating the right atrium and ventricle (this valve is due to its three valve leaflets called "tricuspid valve", from Latin tri = three).
In rare cases, the pulmonary valve leading to the pulmonary circulation can also be affected.