Femoral neck fracture
introduction
A Femoral neck fracture is the fracture of the Throat of the femur, also known as the collum femoris in medical terminology.
The injury usually occurs as a result of a Fall or otherwise Force acting on the femoral neck and is typical for older people. The risk of suffering a femoral neck fracture correlates to a high degree with the individual's tendency to fall, which can be significantly increased due to the factors of old age, frequent circulatory problems with a tendency to collapse or the use of sleep or pain medication.
At young people A femoral neck fracture occurs much less often and is usually on massive violence can be traced back to the thigh bone, as occurs, for example, in trauma in the context of traffic accidents.

Gender distribution of the femoral neck factor
The presence of a osteoporosiswhich is associated with a reduction in bone density and a reduction in bone stability, significantly increases the risk of suffering a fracture of the femoral neck in the event of a fall.
There Women in old age are affected by osteoporosis much more frequently than men of the same age, the Femoral neck fracture more common in women on.
Appointment with a hip expert?

I would be happy to advise you!
Who am I?
My name is I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
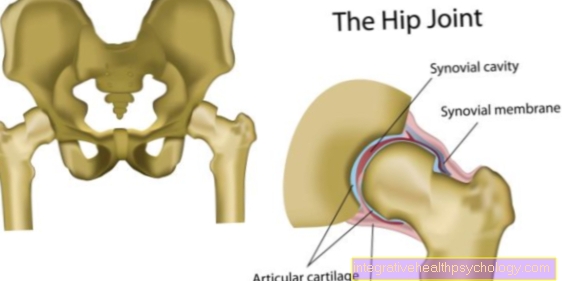
The hip joint is one of the joints that are exposed to the greatest stress.
The treatment of the hip (e.g. hip arthrosis, hip impingement, etc.) therefore requires a lot of experience.
I treat all hip diseases with a focus on conservative methods.
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- - your orthopedic surgeon
14
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
Further information about myself can be found at
causes
The root cause for a fracture of the femoral neck is in any Force acting on the femoral neck to search.
In the young organism, the thigh bone is designed as a supporting component of the musculoskeletal system for extremely high loads. Rotational, bending and shearing forces, such as those that occur when running, jumping, but also with bumps and falls, are easily withstood.
Take the Bone density and thus the Bone stability in older age, usually additionally benefited by osteoporosis even minor traumas, such as falls at home, can lead to a fracture of the femoral neck. In the case of very advanced thinning of the bone substance, a spontaneous break can occur even under normal stress.
Young patients with a healthy bone structureR fractures of the femoral neck usually only suffer under massive violence. Typical are here traffic accidents such as colliding with another car at high speed or falling on a motorcycle.
If a femoral neck fracture occurs young people as a result of a minor trauma or even spontaneously without any special application of force, must contact a abnormal thinning of the bone structure for example in the context of hormonal diseases or one Tumor be thought.
Symptoms
A Femoral neck fracture mostly goes with severe pain which can be increased by attempting to move in the hip joint and especially by applying pressure to the large rolling hillock, the so-called greater trochanter.
Rarely, and especially with collapsed and not displaced fractures, only moderate pain occurs, which can be mistaken for a bruise of the hip. As a rule, however, those affected complain of the greatest pain, which increases with the degree of displacement of the fragments and are no longer able to walk.
For the experienced examiner this is Determination of a femoral neck fracture usually a visual diagnosis, characterized by Shortening and external rotation of the injured extremity. The external rotation is created by pulling the muscles of the buttock muscles that attach to the large rolling hill (greater trochanter). The shortening of the extremity results from the displacement of the fracture line or even from the extremely painful tilting of the femoral head.
Depending on how the accident happened Bruising occur in the area of the hip joint.
Diagnosis
The suspected diagnosis, which is usually due to the Accident mechanism and the typical position of the injured leg can be made, is supplemented by further diagnostic steps. During the physical examination, tenderness on pressure over the large rolling hill and pain on movement when the hip joint is mobilized are examined.
As part of the fracture diagnosis, the blood flow to the lower extremity is controlled by determining the foot pulses and maintaining the sensitivity below the fracture. The receiving doctor also becomes a X-ray of the pelvis and the femoral head.
Classification of the fracture according to Garden and Pauwels
The Classification according to Pauwels takes place via the determination of the Inclination angle of the fault line. It has the greatest relevance in the clinic for assessing the severity and prognosis of the injury.
The division into the three degrees of severity is based on the Angle between fault line and horizontal. Is this between 0 ° and 30 °, one speaks of Pauwels grade I, at 30 ° to 50 ° from Pauwels grade II. At an inclination angle of more than 50 ° one speaks of a shear fracture with the most severe Pauwels grade III.
The increasing severity according to Pauwels indicates an increasing instability of the fracture. Grades Pauwels II and III are always an indication for an operative restoration of the bone, a so-called osteosynthesis.
Also the Garden classification indicates a decrease in fracture stability with increasing severity. The division, which is mainly used in the USA, is different four levels.
Garden I. refers to an incomplete fracture with compression, which is rather stable. There is no displacement of the fragments. At Garden II the break is complete, but the fragments are still touching and are not shifted or rotated against each other. The break is still stable.
Garden III refers to a complete femoral neck fracture in which the fracture fragments are shifted against each other and the femur shaft is rotated relative to the fracture near the body, but still have contact. This contact is at Grade IV according to the Garden classification, the fracture fragments do not touch at any point, a pronounced dyslocation is present.
The The prognosis for Garden I and II is good, whereas patients with existing femoral neck fractures are classified with Garden III and IV one supplied surgically should be.
therapy
As can be seen in the previous section, surgical treatment of a femoral neck fracture is not always necessary.
The necessity derives from the described division into Garden classification systems and Pauwels is always a case-by-case decision, taking into account factors such as the patient's age and symptoms.
A conservative treatment, that is, one Treatment without surgery, as can already be seen from the recommendations for the individual classification systems, is ideal for stable or wedged fractures (Pauwels I and Garden I to II). Conservative treatment consists of one Use it to immobilize the affected extremity the broken bones underneath can grow back together. If the immobilized bone ends shift in the course of conservative treatment, surgery should be sought immediately.
In order to keep the physical consequences of immobilization as low as possible, especially in older people, a Mobilization of the affected extremity be done under professional guidance.
If an unstable fracture is treated conservatively due to inoperability of the patient, although surgical treatment would be indicated, attention must be paid to a sufficiently long immobilization and an effective prophylaxis of concomitant diseases such as thrombosis or embolism.
The Surgery for a femoral neck fracture is suitable for unstable fracture conditions and is characterized by better stability and shorter immobilization out. The appearance of complications with long conservative treatment of unstable fractures usually makes surgery necessary. In an emergency, this should be done within six hours of the injury. For patients of younger age, the restoration can be carried out with a dynamic hip screw (DHS) while preserving the femoral head. The injured extremity is brought into the correct position before the operation and the fracture is then placed through a skin incision with the using X-ray technology Hip screw fixed.
In patients over 65 years of age, the Implantation of a hip prosthesis be considered. During this operation, the femoral head and, in some cases, the acetabulum are completely replaced by artificial structures. The loading can begin relatively soon after the operation, so that complications from long immobilization are avoided as far as possible.
forecast
An early one Mobilization of the patient is the key element of successful treatment. Especially at an advanced age, the femoral neck fracture can lead to life-threatening circumstances, for example if Blood clots or pressure sores occur as complications of long immobilization during conservative treatment or after surgery. Pneumonia also occurs more frequently after long-term hospital treatment.
All of these complications can be eliminated by a early care of the patient through the physical therapy in the rehabilitation phase (Rehabilitation after a femoral neck fracture) can be effectively avoided. Adequate pain therapy enables the affected extremity to be mobilized promptly, which is usually guided by the physiotherapist for two to three weeks. The discharge from inpatient treatment is usually followed by follow-up treatment.
prophylaxis
In order to prevent a femoral neck fracture, the main cause, a general tendency to fall, must be eliminated or reduced, especially in older people.
In addition to circulatory problems that can lead to collapse, the triggering factors for falls are also Overdose or incorrect intake of sleep, pain or sedation medication. Especially when medication with many different drugs should be Medication schedule critically examined for interactions between the individual preparations.
At existing gait uncertainty A supply of walking aids and extensive training in their use should also be provided in the home environment. In individual cases, the apartment must be examined for accessibility and its suitability for the elderly resident and, if necessary, converted. Trained nursing staff in home care often recognize “tripping hazards” such as carpets or doorsteps and can help with them everyday environment safe to design.
Especially in women of advanced age is a so-called Bone density measurement helpful to an existing osteoporosis to recognize and e.g. by taking Calcium and Vitamin D Supplements to prevent progress. Men also occasionally develop osteoporosis. In both sexes, the disease can be favored by taking certain medications.