Infarct pneumonia
What is infarct pneumonia?
Infarct pneumonia is a special form of pneumonia that occurs after what is known as a pulmonary embolism. It is therefore to be regarded as a complication of the pulmonary embolism. The term pulmonary embolism is used in medical jargon for an acute infarction of the lung tissue that results from an occlusion of the pulmonary arteries. This occlusion is usually the result of a leg vein thrombosis. The blood clot is usually carried via the vascular system from the leg veins to the pulmonary arteries, where it causes an infarction, similar to a heart attack. Infarct pneumonia is a rather rare complication of pulmonary embolism that requires antibiotic treatment.

Causes of Infarct Pneumonia
Infarct pneumonia occurs as a complication of a pulmonary infarction. Pulmonary infarction as such is usually the result of a pulmonary embolism, which is an acute occlusion of the pulmonary arteries. This blockage is usually caused by blood clots, so-called thrombi, in the leg veins, which can be carried via the venous system into the heart and from there into the lungs.
Pulmonary infarcts and, as a consequence, infarct pneumonia also occur less often due to the establishment of a central venous access in the hospital (central vein catheter) or due to fat embolism. The latter are mainly complications of major surgical interventions, such as the insertion of endoprostheses. Infarct pneumonia occurs due to a very distant occlusion of the pulmonary arteries. Such an occlusion means that blood flow to the lung tissue can no longer be maintained and the tissue becomes necrotic - it thus dies. Bacteria can now easily penetrate the tissue and cause pneumonia there.
Also read the article on the topic: What are the consequences of a pulmonary embolism?
Pulmonary embolism
A pulmonary embolism is an occlusion of the pulmonary artery, which is usually caused by so-called thrombi. These types of blood clots are most common in the leg and pelvic veins. Such blood clots can be carried through the bloodstream into the heart and then further into the pulmonary arteries. There they then cause an embolism, i.e. an occlusion of the pulmonary artery.
People with a so-called thrombophilia, i.e. a predisposition to the formation of blood clots, are particularly at risk. Furthermore, other factors, such as smoking, long bed rest, operations or pregnancy, promote the risk of such a thrombosis and, as a consequence, a pulmonary embolism. If arteries located very far outside in the lung tissue are blocked, a pulmonary infarction can occur. The blood flow to the tissue is then completely interrupted, so that wedge-shaped infarcts occur and the lung tissue dies. Infarct pneumonia can then develop as a complication in such an area.
Read more on the topic: Pulmonary embolism
What are the symptoms of infarct pneumonia?
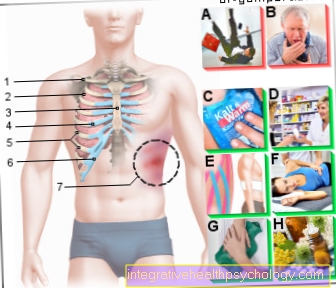
Infarct pneumonia typically leads to an increase in fever and general fatigue. Cough and purulent sputum may also be present. The sputum then often has a yellowish or green color, but it can also be completely absent. Furthermore, an increased respiratory rate and shortness of breath can indicate infarct pneumonia. An increase in heart rate, i.e. tachycardia, is also typical and can manifest itself as restlessness and nervousness.
Headache and body aches are typical symptoms of infarct pneumonia. Pain in breathing can also be one of the symptoms of infarct pneumonia as a result of an accompanying inflammation of the lung membrane, a so-called concomitant pleurisy. Frequently, however, the symptoms appear in a weakened form, so that one also speaks of a subclinical course. Often only an increase in fever after a pulmonary embolism is an indication of the presence of infarct pneumonia.
diagnosis
The diagnosis of infarct pneumonia is based on clinical symptoms and imaging techniques. Initially, there is usually a pulmonary embolism, which can be detected using a so-called CT angiography. This is a CT examination of the pulmonary vessels with a contrast medium. Symptoms such as shortness of breath, chest tightness and an increase in heart rate also suggest pulmonary embolism.
Also read the article on the topic: How can you recognize a pulmonary embolism? What are typical signs?
If the fever rises and general fatigue after a pulmonary embolism, infarct pneumonia is suspected, so that the diagnosis can then be made using an X-ray of the lungs. Typical changes that indicate infarct pneumonia can be seen in the X-ray image (see the X-ray section). A blood test can often be used to determine increased infection parameters in infarct pneumonia. These include increased CRP and PCT levels, as well as increased white blood cells. These values indicate in particular that there is a bacterial infection.
roentgen
If infarct pneumonia is suspected, an X-ray image of the chest is made. Typically there are changes in the lung tissue that are also known as Hampton's hump. This is a wedge-shaped decrease in the transparency of the lungs that is on the outside of the lung tissue. This reduction in transparency appears white in the X-ray image. One also speaks of a wedge-shaped or triangular infiltrate of the lung periphery.
Treatment / therapy
Infarct pneumonia must be treated in any case, as it is a serious clinical picture. Infarct pneumonia is usually treated as an inpatient because the lungs have previously been damaged. In the treatment of infarct pneumonia, the main focus is on antibiotic therapy. Antibiotics can be used to kill the bacteria that cause pneumonia. In clinical practice, the active ingredients ampicillin / sulbactam are often used in combination with a macrolide antibiotic such as clarithromycin. This combination covers the typical pathogens of infarct pneumonia. In very severe infarct pneumonia, more potent antibiotics such as piperacillin / tazobaktam are used.
The choice of antibiotic depends on the severity of the infarct pneumonia, as well as other factors, such as the age of the person affected, other previous illnesses and the general condition. Antibiotic treatment is carried out as intravenous therapy with infusions. For this, the patient needs a vein access. Furthermore, antipyretic drugs such as paracetamol are used in the treatment of infarct pneumonia. At the same time, fluids are administered via the venous access to prevent the patient from drying out.
Antibiotics
Infarct pneumonia occurs due to a bacterial infection. Common pathogens of infarct pneumonia are pneumococci, chlamydia or mycoplasma. The bacteria Pseudomonas aeruginosa, enterobacteria and staphylococci are also found in hospital-acquired pneumonia. The antibiotic treatment is determined based on the patient's risk profile. The risk profile is determined by the age of the patient, relevant previous illnesses and whether the infection arose in the hospital or on an outpatient basis, i.e. outside the hospital.
In any case, however, antibiotic treatment is necessary to kill the germs. A combination of the antibiotics ampicillin / sulbactam and clarithromycin is often used. This combination covers as many pathogens as possible. For very severe infarct pneumonia, a combination of piperacillin / tazobaktam and clarithromycin is used. The antibiotics levofloxacin and moxifloxacin are also commonly used. The antibiosis will be adjusted as soon as the pathogen is detected. The most effective antibiotic is selected based on the pathogen detection.
Course of disease
Infarct pneumonia often manifests itself through rather discrete complaints and general fatigue. If there is no therapy, the patient's condition worsens and permanent damage to the lungs or even sepsis, i.e. the bacteria being washed out into the bloodstream with organ failure, are possible.
After starting antibiotic therapy, the patient's condition improves within a week. In the case of severe pneumonia, however, the therapy must usually be carried out for 14 days and in any case for at least a further 3 days after defever. A feeling of exhaustion can persist a little longer.
Duration / forecast
The prognosis of infarct pneumonia depends largely on the condition and previous illnesses, as well as the age of the patient. The prognosis worsens with age. Infarct pneumonia acquired in hospital has a mortality rate of up to over 20%. Older people in particular are at great risk from this so-called nosocomially acquired infarct pneumonia.
Treatment should therefore not be delayed under any circumstances. Younger patients who got pneumonia outside of the hospital, on the other hand, have a good prognosis if therapy is carried out consistently.
How contagious is infarct pneumonia?
Infarct pneumonia occurs due to previous damage to the lungs, which usually occurs as part of a pulmonary embolism. This pre-existing damage promotes pneumonia. The pathogen is transmitted via droplet infection. This means that those affected cough up the pathogen or spread it in the air with a sneeze. In the event of contact, the pathogens can also be absorbed through the breath.
Nevertheless, people with an intact immune system are not particularly at risk of contracting an affected person. Older people and small children in particular should avoid contact with those affected until antibiotic therapy has been given for a sufficient period of time. In the event of contact, it is advisable to wear a mask and gloves to keep the risk of infection as low as possible. Unfortunately, the duration of the risk of infection cannot be given across the board, so that the doctor treating the person concerned should be asked about this in any case.
Also provide information on the topic: How contagious is pneumonia?











.jpg)