lung
definition
The lungs (pulmo) are the body's organs that are responsible for adequate oxygen intake and supply. It consists of two spatially and functionally independent lungs and with these surrounds the heart. The two organs lie in common in the chest (thorax), protected by the ribs. The lungs do not have their own shape but are shaped in their relief by the surrounding structures (diaphragm below, heart in the middle, outside the ribs, above the windpipe and esophagus).

Structure of the air-conducting airways
The easiest way to understand the anatomy of the lungs is to follow the path of the air we breathe:
Through the mouth or the nose the air gets into the body. Then it flows into the throat (Pharynx), then into the Larynx (larynx) with the vocal folds.
Up to this point, the air and food routes are identical. The begins at the passage between the vocal folds, which form the narrowest point in the upper airways windpipe (Trachea).
In the anesthesia and in the case of emergency patients, this bottleneck is bridged by a tube (ventilation hose) (Intubation) to supply by a machine Ventilation to be able to secure. From the vocal folds onwards, all of the following sections are purely air-conducting; if foreign objects get here, one speaks of one aspirationwhich then triggers the cough reflex.
Anatomy of air ducts

- Right lung -
Pulmodexter - Left lung -
Pulmo sinister - Nasal cavity - Cavitas nasi
- Oral cavity - Cavitas oris
- Throat - Pharynx
- Larynx - larynx
- Windpipe (approx. 20 cm) - Trachea
- Bifurcation of the windpipe -
Bifurcatio tracheae - Right main bronchus -
Bronchus principalis dexter - Left main bronchus -
Bronchus principalis sinister - Lung tip - Apex pulmonis
- Upper lobe - Superior lobe
- Inclined lung cleft -
Fissura obliqua - Lower lobe -
Inferior lobe - Lower edge of the lung -
Margo inferior - Middle lobe -
Lobe medius
(only on the right lung) - Horizontal cleft lung
(between upper and middle lobes on the right) -
Horizontal fissure
You can find an overview of all Dr-Gumpert images at: medical illustrations

- Bronchiole
(cartilage-free smaller
Bronchus) -
Bronchiolus - Branch of the pulmonary artery -
Pulmonary artery - End bronchiole -
Respiratory bronchiolus - Alveolar duct -
Alveolar duct - Alveolar septum -
Interalveolar septum - Elastic fiber basket
of the alveoli -
Fibrae elasticae - Pulmonary capillary network -
Rete capillare - Branch of a pulmonary vein -
Pulmonary vein
You can find an overview of all Dr-Gumpert images at: medical illustrations
The windpipe is very far forward in the neck, so that there is the possibility of making a trachea incision (Cricothyrotomy). This ensures access to the lungs in the event of an obstruction of the upper airways (e.g. vomit).
The wall of the windpipe consists of the ciliated cells typical of the respiratory tract. These ciliated cells have fine hairs (kinocilia) on their surface, with which they transport mucus and foreign bodies (e.g. bacteria) towards the mouth towards the throat.
The mucus contains special antibacterial (against bacteria) substances and is formed by another specialized cell type (so-called goblet cells).
It has a mechanical and immunological (bacterial defense) protective function. Various causes, especially cigarette smoke (smoking), lead to irritation of the ciliated cells and increased mucus formation.
The approx. 20 cm long windpipe finally branches in the chest into a left and right main bronchus (Bifurcatio tracheae), which then lead into the right and left lungs respectively. The right bronchus (= branch of the pleasure tube) is slightly larger and runs at a steeper angle, so that swallowed foreign bodies are more likely to get into the right lung.
The point at which the Bronchi entering the lungs is called the hilus; the blood and lymph vessels also enter the lungs here.
Structure of the lungs
In the lungs, the bronchi undergo a total of more than 20 divisions: First, a distinction is made between three lobes on the right and two on the left, which can be further subdivided. The walls of the bronchi contain cartilage clips and smooth musculature (Bronchial muscles), with the stock of cartilage rods continuously decreasing with greater distance from the mouth.
The Cartilage braces have the task of preventing the bronchi from collapsing during inhalation (negative pressure in the lung tissue!). As they run through the lung tissue, the bronchi are accompanied by the pulmonary arteries with the deoxygenated blood from the right heart.
In contrast to this, the veins with the oxygen-rich blood run in the boundaries between the individual lung segments. This is important insofar as the surgeon can easily find his way around the lung tissue and, if necessary, can remove individual segments without loss of function of the remaining tissue (partial lung resection).
The end of the branches of the airways are the Air sacs (alveoli). Although they are very small (diameter well below 1 mm), they are so numerous (an estimated 300 million pieces) that their total surface is as large as a tennis court.
If the total surface area of the alveoli, which is important for gas exchange (oxygen in - carbon dioxide out), is reduced, one speaks of one restrictive ventilation disorder. Symptoms of this disease are shortness of breath and an accelerated breathing rate, since not enough oxygen can be absorbed per breath due to a lack of space.
The individual alveoli are grouped like grapes around the smallest extensions of the bronchi. Since they do not have an air-conducting, but air-exchanging task, they have a special wall construction. The cells are particularly thin and no longer have the cilia that are typical of the respiratory tract.
There are other special cells in the alveoli wall. Their job is to form surfactant, a mixture of fat and protein that is responsible for reducing the surface tension in the alveoli.
The surface tension is the force that prevails at the air-liquid boundary between the alveoli wall with the mucous layer on the one hand and the air space inside the alveoli on the other. The surface tension gives the alveoli a tendency to contract. This tendency is favored by the numerous elastic fibers in the lung tissue, which stretch when you inhale and which act as the driving force for exhalation.
Tiny blood vessels (capillaries), but not lymphatic vessels, run in the walls of the alveoli and the smallest bronchi. This makes it more difficult for the body to do the job of the lymphatic system (removing fluid).
Therefore, an accumulation of fluid in this area (pulmonary edema) leads to a significant impairment of function.
The blood vessels transport the used blood and release the end product of metabolism (carbon dioxide; CO2) in the alveoli. At the same time, they take in fresh oxygen and enter the great circulation via the left heart. This gas exchange takes place in a contact time between blood cells and alveolar wall of only 0.3 seconds!
If you follow the path of air again, you will see that all airways have a direct connection with the environment; there is no barrier between the lips and the inner lining of the alveoli.
Since 500 ml of air are inhaled per breath (about 12 times per minute), one can imagine that the lungs are intensely confronted with viruses, bacteria and fungi from the environment.
Furthermore, the lung tissue with its mucous layer offers excellent growth conditions for pathogens of all kinds. In all sections of the respiratory tract one can find cells of the body's own defense system (immune system), some of which try to ward off this hazard directly, some through released products. Failure to do this can lead to inflammation of the air-conducting systems (bronchitis) or, worse, pneumonia itself.
Also read our article: Foreign bodies in the lungs - This is what you should be doing

Anatomy and location of the lungs
- Right lung
- Windpipe (trachea)
- Tracheal bifurcation (carina)
- Left lung
Suspension of the lungs
The lungs are surrounded by a kind of skin, the Lung membrane (pleura).
The lung membrane consists of two leaves that merge into one another at the entry point (hilus) of the lungs. The inner sheet (Visceral pleura) is very close to the actual lung tissue. The outer leaf (parietal pleura) lines the chest (thorax) from the inside, creating a tiny gap between the two leaves.
This gap, also called the pleural gap, is filled with a few milliliters of fluid. As a result, the lungs are stretched across the chest and cannot collapse. On the other hand, the lungs are breathable in relation to the chest.
Pleural space
Everyone knows the phenomenon at home: If you press two glass plates with water between them, you can move them against each other - you can't separate them.
This is how the pleural space works!
The lung tissue tends to collapse due to elastic fibers, but is attached to the chest by the lung membrane. Overall, there is a negative pressure in the gap between the two lungs.
If there are injuries to the chest or a tear in the lung tissue, air flows into the gap between the two leaves and the lungs collapse; the clinical picture of Pneumothorax.
Further information is available under our topic: Pneumothorax.
Due to various causes (Heart failure (Heart failure), tumors, inflammation), more fluid can also get into the pleural space.
In this case one speaks of a Pleural effusion.
The effusion usually collects at the deepest points of the pleural space, namely in the lateral angles between the diaphragm and the ribs. In both cases, breathing is difficult.
The lungs become very fine from annoy that can guide pain. Injuries involving the pleura are therefore very painful. In contrast, the lung tissue is unable to feel pain due to the lack of nerve tracts.

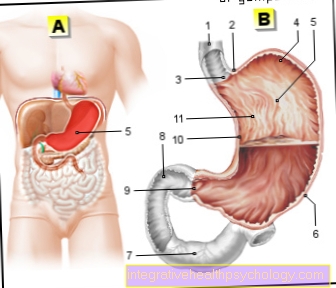
Structure of the thorax
- Collarbone
- rib
- lung
- Chest wall
- heart
- diaphragm
- liver
- Mediastinum
- Skin artery (aorta)
- Upper vena cava (vena cava)
A cut was made here parallel to the forehead (frontal cut), which even hits the intestines. Both lungs are cut, the heart, which was partially covered by the lungs, is now visible in all its glory. In addition, the multi-storey structure of the trunk becomes clear: under the thorax lies the abdominal cavity with liver and stomach, the border is the diaphragm.
Mechanics of breathing
The lungs are not an independently moving muscle, but rather a hollow organ with a large exchange surface that needs to be "ventilated". For this purpose, the lungs are at the so-called Pleurathat is on the chest. There are strong muscular connections between the ribs of the chest. With every breath they pull Muscles between the ribs together and that diaphragm contracts, causing the diaphragm to flatten. Since the pleura is also connected to the diaphragm and the ribs, the muscles work to expand the chest. With this chest enlargement, the lungs attached to the chest are expanded. This expansion becomes by a negative pressure the necessary air is drawn into the lungs and gas exchange takes place in the alveoli.
You can find more information on this topic here: breathing
Diseases of the lungs
Collapse of the lungs
Despite the very stable connection between the lungs and the inside of the chest, parts of the lungs may become detached and collapse. This is mostly the case when there is a connection between the pleural space, in which there is negative pressure, and the outside air. A connection lets the negative pressure escape to the outside and loosens the adhesion of the lungs, which then collapse. This connection between the plaura gap and the outside air is known as the pneumothorax. Most often, a pneumothorax develops after a medical procedure in which e.g. excess water is punctured from the pleural cavity. In this case, the pleural space is accidentally pierced by the practitioner's needle, the air flows in and relieves the negative pressure in the pleural space, which can then lead to a collapse of the affected lung.
But it can also occur just like that, especially in sporty young men, this is then referred to as spontaneous pneumothorax.
The first signs of pneumothorax are shortness of breath, malaise, and a fast beating heart. Sometimes a pneumothorax can cause no symptoms at all and only become noticeable in the x-ray of the lungs.
Read more on the topic: Chest x-ray (chest x-ray)
While a simple and unilateral pneumothorax should be treated promptly, bilateral pneumothorax or tension pneumothorax is an absolute emergency. In tension pneumothorax there is a type of valve so that air from the outside can enter the pleural space when inhaled, but cannot escape again . With every breath, the amount of air in the pleural space increases, so that the internal organs and especially the heart are pushed to the side of the collapsed lungs, which can lead to severe circulatory restrictions. To treat a pneumothorax, a drain is pushed into the pleural space from the outside, thereby restoring the negative pressure. This then leads to the lungs expanding again, which can then be ventilated normally again.
Changes in the lung tissue, e.g. pneumonia or obstructions of the bronchi can lead to collapse of sections of the lungs. This is then known as atelectasis.
Burning in the lungs
A burning sensation felt by the patient in the area of the lungs different causes to have.
In the case of inhaled toxic substances, e.g. of poisonous smoke after a fire, there is almost always one Irritation of the very sensitive epithelium of the bronchi. The Smoke inhalation can mean a life-threatening condition. The longer a person has been exposed to toxic fumes or gases, the greater the risk that poisoning will occur throughout the body. The person concerned usually notices these irritations through burning sensation on inhalation and exhalation.
Much more often there is a burning sensation when breathing in and out after a long bronchitis. Particularly stubborn to cough the epithelium of the lungs becomes irritated, which the person concerned registers with a burning sensation when inhaling and exhaling. Most of the time the burning sensation lasts until the persistent cough has either disappeared or the dry cough has turned into a slimy cough.
After a Clarification of the cause a doctor can relieve the burning sensation in the lungs through various measures. For one, should tight mucus through medication like ACC or NAC be solved. Alternatively or in addition to this, a Steam inhalation be performed. For this you would fill a pot with water and something Chamomile extract do this. After that, the mixture is brought to a boil, taken off the stove and inhalation is then started with a towel over the head. The inhalation should take approx Last 10-15 minutes and 2 times a day be performed. Through the steam inhalation, the chamomile extract comes through the finest droplets into the lungs and thus leads to a Anti-inflammatory of the epithelium of the burning bronchi. With regular use, symptoms should improve within a week.
Cleaning the lungs
There is no actual lung cleansing. However, there are some behaviors that can ensure that toxins and tar substances that have accumulated in the lungs over time are slowly washed away. These measures must regularly can be applied and a positive effect occurs only after a long period of time on.
The first measure that should be carried out in the best possible way is to reduce the inhalation of toxins, which of course also includes quitting smoking or reducing passive smoking.
After that, a Steam inhalation carried out, which ensures that the sensitive lung epithelium regenerates and the inflammation present there dissolves more quickly. By clean air to breathe the lungs can regenerate faster. Especially traveling in Mountain regions or the sea ensure that clean air can be breathed at least for the duration of the trip. There is also the option in artificial salt tunnels or salt caves where you can do a salt inhalation. This measure also leads to faster regeneration and "cleaning of the lungs"
Lung puncture
A distinction is made between those that are carried out frequently Pleural puncture from the somewhat less frequently carried out Lung puncture.
A pleural puncture can easily be performed and takes place whenever Fluid in the pleural space accumulates and presses on the lungs. After prior ultrasound control and under sterile conditions, the pleura is pierced from the outside with a small needle and the fluid is drained through the needle.
The rarer one Lung puncture always takes place when a suspicious finding or focus in the lungs but the exact cause is unknown. A lung puncture is always carried out using a CT scan and is intended to Tissue samples from the suspicious hearth for closer investigation. To do this, a CT-A recording is made and the suspicious findings are displayed, so then by means of a Puncture needle pierce the chest wall and lungs be to hit the stove. The procedure takes depending on the location of the focus a few minutes up to half an hour.
If such suspicious foci are in the vicinity of large bronchi, an attempt is made to pass the samples through a Lungoscopy (bronchoscopy) to win so as not to injure the chest.
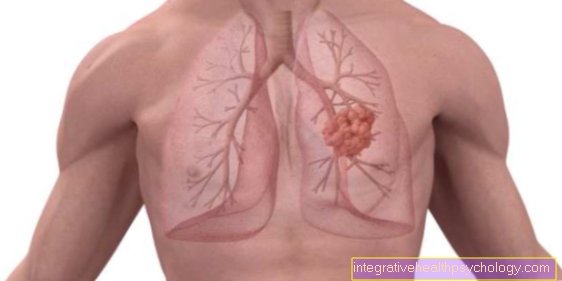
If lung cancer is suspected, samples are often obtained by puncturing the lung.