Subacromial decompression / shoulder roof expansion
Synonyms
ASD, SAD, OAD, shoulder decompression, subacromial decompression, rotator cuff, rotator cuff tear, calcar tendinosis
definition
The so-called subacromial decompression expands the area below the acromion (= sub acromial = shoulder roof), whereby a normal sliding process of the rotatorem cuff below is guaranteed. The subacromial shoulder roof enlargement is carried out in the shoulder constriction syndrome (impingement syndrome).
There are basically two methods of surgical therapy:
- Arthroscopic subacromial decompression (ASD)
- Open subacromial decompression (OSD)

Appointment with a shoulder specialist

I would be happy to advise you!
Who am I?
My name is Carmen Heinz. I am a specialist in orthopedics and trauma surgery in the specialist team of .
The shoulder joint is one of the most complicated joints in the human body.
The treatment of the shoulder (rotator cuff, impingement syndrome, calcified shoulder (tendinosis calcarea, biceps tendon, etc.) therefore requires a lot of experience.
I treat a wide variety of shoulder diseases in a conservative way.
The aim of any therapy is treatment with full recovery without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- - your orthopedic surgeon
14
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
You can find more information about myself at Carmen Heinz.
Arthroscopic subacromial decompression (ASD)
Arthroscopic subacromial decompression - ASD - is performed using two small skin incisions as part of one performed simultaneously Arthroscopy (Reflection) of the Shoulder joint. The two skin incisions are made above the actual shoulder joint interior.
Operational additions

As already mentioned, you only need two small incisions in the skin for access.
Two entrances are necessary, one being the so-called optics must be introduced (rear access), on the other hand, the surgical instruments must also be introduced (side access). The optics represent a small camera that displays images of the shoulder on an external monitor. As part of an ASD, surgical instruments can be, for example, electric knives or shavers, which are required to expand the area.
Further information is also available at Arthroscopy.
Operational approach
The procedure is divided into 2 steps: Bursoscopy and subacromial decompression
- The so-called bursoscopy is a form of diagnosis. The subacromial bursa (bursa) is examined and assessed using the optics. The optics, which are pushed from the back of the shoulder under the acromion into the subacromial bursa, can be used to detect any adhesions, thickening or reddening, which ultimately affect the second step, subacromial decompression.
The condition of the rotator cuff can also be assessed using buroscopy. To do this, the optics are aligned "downwards". Rotator cuff tears are easy to recognize because the bursa itself lies on the rotator cuff and is fused with it.
A look "upwards" enables a visualization of the lower surface of the acromion. This is the area that, through partial removal, is intended to provide an extension of the subacromial space. This partial removal is carried out by means of a shaver, which removes this bone area by turning and cutting movements. This process takes place as part of the second step described below. - The actual subacromial decompression consists of two sub-steps, the removal of the soft tissues and the bone resection.
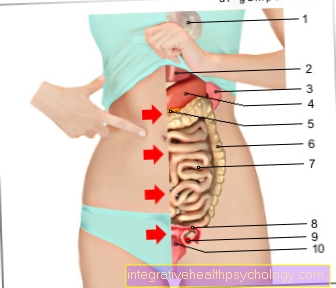
As part of the soft tissue removal, thickened parts of the bursa (mucous sac -> see picture) are removed and the soft tissues on the underside of the acromion (underside of the canopy) are removed. This soft tissue removal is carried out using a shaver. Since cuts in these areas always bleed and bleeding worsens the view, hemostasis with an electric knife is always necessary to obliterate the bleeding.
Bone resection involves milling away the bone on the underside of the acromion. The shaver is also used for this, but the attachment is changed.
During the operation, the acromion was thinned and a large part of the soft tissue and the bursa were removed. A widening of the subacromial space can be seen, so that the newly created distance between acromion and rotator cuff now enables better sliding movement.

Figure shoulder roof spur
Before the operation
Image of a special x-ray image (outlet view), in which one can see a constricting spur under the shoulder roof, which damages the rotator cuff and ultimately leads to a tear in the rotator cuff.

Result after operative care
After the operation
The same X-ray after arthroscopic surgery after the spur was removed.
The cause of the tightness was removed. This operation can be performed with the keyhole technique, i.e. in an arthroscopy, without large incisions.
Open subacromial decompression (OSD)
The second possibility of an operative intervention is the open subacromial decompression, which was used as the only possibility of the operative enlargement operation before the standardized use of the ASD.
In contrast to the ASD, a larger skin incision (about 5 cm in size) must be made to allow access to the surgical area.
While a reflection of the area to be operated is made within the framework of the ASD, the direct operation begins within the framework of the OSD. The operation itself is traditionally divided into two parts.
In the first part of the operation, the ligament connections between the acromion and the coracoid are removed. This loosening of the band connections can be done individually in different ways. Not all tape connections always have to be loosened. In some cases, tape connections are also re-fixed later.
Following the first partial step of the OSD, the second partial step is to remove the bony wedge on the underside of the acromion.
A reduced distance between the acromion and the humeral head should be increased in order to allow the rotator cuff sufficient freedom of movement.
Now the first step of the OSD takes place: The tape connections between Acromion and Coracoid are removed.
The second step, the removal of the bony wedge, is then used.
In the context of the OSD, a chisel is required instead of a shaver (see ASD).
Operational additions
The procedure consists of 2 parts in the classic way:
- Remove the ligament connection between acromion and coracoid (ligamentum coraco-acromiale).
- Removal of a bone wedge of a certain size from the anterior lower surface of the acromion
Decompression Risks
The risks of subacromial decompression depend on a number of factors. The expression of the impingement syndrome has an effect on the chances of recovery and the improvement after the operation despite the operation. The two different surgical procedures also entail different risks. In general, the arthroscopic approach is very low-risk. Nevertheless, before the operation, all potential consequential damage and side effects of anesthesia and the operation must be clarified.
Since subacromial decompression is usually performed under general anesthesia, the first risks can arise during the anesthesia. In addition to intolerance and allergies to the anesthetic, irritation from the ventilation tube in the windpipe can also occur. This can cause hoarseness and a sore throat.
The risks of the actual operation include, among other things, accidental damage to the structures being operated on. If the joints are unstable, particular care must be taken during surgery, as severing ligament structures can exacerbate the instability. In addition, there is a risk of injuring the muscle and bone structures of the shoulder joint, as well as cartilage surfaces and joint parts. This can lead to bruises in the surgical area. Under certain circumstances, there is a risk that the operation that has been carried out will bring about little or no improvement.
With all invasive procedures, whether minimally invasive or as open surgery, there is a risk of infection by pathogens. By cutting through the skin barrier and opening the operating area, pathogens can penetrate and inflame the shoulder region, muscles, wound site and skin if there is insufficient hygiene. This is one of the reasons why the patient has to spend a few days in the hospital even after a positive operation.
Subacromial decompression pain
There will initially be pain before and after the operation. Painful impingement syndrome is the most common indication for subacromial decompression. In the days after the operation, slight pain in the wound and surgical area may reappear. An operation always results in minor injuries to the soft tissues and the operated structures. Small blood vessels are also often injured, which can lead to minor bruises in the shoulder joint. These are sometimes painful, but should not last longer than a few days to a few weeks. The actual pain caused by impingement syndrome shouldn't recur after surgery. Medication such as ibuprofen or paracetamol can be taken temporarily for mild surgical pain.
Aftercare
Cooling measures (cryotherapy measures) are taken immediately after the operation to reduce the pain and, above all, to reduce the swelling of the soft tissue. In addition, pain relievers and decongestants can be prescribed individually as required.
A so-called Redon drainage can be inserted to allow the wound secretion to drain from the operated area. This drainage is removed about one to two days after the operation.
In the first few days, the arm is usually immobilized with the help of an arm sling.
In order to bring the arm back to movements as quickly as possible and to ensure it, physiotherapeutic follow-up treatment is prescribed from the 1st postoperative day. This includes, on the one hand, so-called passive movements, which the physiotherapist performs in the lead, and, on the other hand, after a certain lead time, active movements that the patient performs himself under physiotherapeutic guidance.
In addition, there is the possibility of post-treatment with the help of a motor movement rail (= CPM). While the patient is sitting in a chair, the shoulder is placed on an electrically powered movement rail and a pain-free movement of the shoulder is initiated. Patients generally find treatment with CPM pleasant. The movement rail can be adjusted continuously and according to your individual scale.
Sick leave after subacromial decompression
The duration of sick leave after subacromial decompression must be made dependent on the healing success. Freedom of movement in the arm must also be fully restored, which can take several months. The sick leave also depends on whether a physical activity is carried out or not.
The average process after the operation shows that the joint in a bandage is completely immobilized and unable to move for about 1-2 weeks. During this time, the arm should be completely spared; household help may be necessary. Movement is then restored, which is achieved with light physiotherapy without stressing the shoulder joint. Full mobility and resilience should be aimed for after about 3 months. Only then may throwing or punching sports, as well as swimming, be practiced again.
The sick leave also varies. In the case of light office work, a return to work can sometimes take place after 2 weeks. If the function of the arm is required in full at work, 2 months' sick leave may be necessary.