Diagnosis of Crohn's disease
introduction
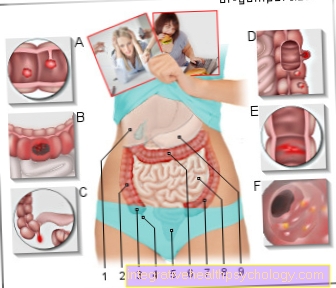
Crohn's disease is a chronic inflammatory bowel disease that manifests itself in many different ways. Since it can appear differently for each person affected, this is Diagnosis is often difficult.
The Life expectancy is hardly or not at all restricted in patients with Crohn's disease who receive optimal therapy.

Not every patient has the same symptoms and not every symptom alone is indicative of Crohn's disease. Many symptoms can therefore have a completely different cause.
Read detailed information on the topic: Symptoms of Crohn's Disease
A comprehensive diagnosis is therefore irreplaceable. The various diagnostic tools include an extensive one anamnese (Patient history) who physical examination, the determination of selected laboratory parameters, imaging procedures such as MRI and roentgen, and last but not least Endoscopy and biopsy (Tissue extraction for laboratory examination). A gastroenterologist can then diagnose Crohn's disease by reviewing the findings. Important differential diagnoses that must be distinguished from Crohn's disease are the Ulcerative colitis (Inflammation of the lining of the colon with ulceration), one Diverticulitis (Inflammation of intestinal wall protuberances) and that Irritable bowel syndrome. In an acute case, a Appendicitis be excluded.
Diagnosis with the help of laboratory values
Some laboratory values provide diagnostic evidence of Crohn's disease. The blood gives first indications of an existing inflammatory process in the body. Are during an acute flare-up of Crohn's disease Markers of inflammation as the CRP (C-reactive protein) and the BSG (Sedimentation rate) in blood elevated.
As the body's immunological response to chronic inflammation, it can become a rise of the white blood cells come. This is called Leukocytosis designated. Because the Intestinal lining in Crohn's disease is inflammatory changed, some can nutrient only bad from the intestines absorbed become. The concentrations of Vitamin B12 (Cobalamin) and Vitamin D.
A deficiency in these vitamins confirms the suspicion of Crohn's disease. Vitamin B12 is important for the production of various blood components. When there is a deficiency of vitamin B12, a special form of Anemia, the so-called pernicious anemiabecause only insufficient red blood cells (erythrocytes) can be produced.
If there is a pronounced deficiency, they are also white blood cells and the Platelets affected. It comes to one Leukopenia or. Thrombocytopenia. Anemia in Crohn's disease can also be caused by a Iron deficiencyl occur when iron can no longer be easily absorbed by the intestine. This is also known as Malabsorption of iron.
It can also be done through the inflammation even too Blood loss come, which in turn presents itself as anemia in the laboratory. The laboratory changes described are of a rather unspecific nature and can also occur in other inflammatory bowel diseases. However, those found in the blood are specific to Crohn's disease Antibodies against Saccharomyces cerevisiae, short ASCA. Elevated levels of these antibodies can be found in the blood of around 60% of those affected. The constellation of positive ASCA value and negative value for is even more specific anti-neutrophil cytoplasmic antibodies, p-ANCA for short.
Diagnosing Crohn's disease using stool samples
Based on Stool samples blood loss through the intestines can be determined quickly and easily. The is particularly suitable Hemoccult Test (Guaiac test). This can be used to determine even the smallest amounts of blood in the stool. This occult (hidden) blood, invisible to the eye, is detected using a simple test. However, blood in the stool is not a specific indicator of Crohn's disease. It only corroborates an existing suspicion. In addition, stool samples can be used to detect bacteria how Campylobacter, Yersinia, Salmonella or Shigella.
As well Adeno-, Noro-, or Rotaviruses can be proven. These can, for example, cause intestinal inflammation and symptoms that look like Crohn's disease.
Detection of the relevant intestinal pathogens therefore leads to the exclusion of the diagnosis of Crohn's disease. Often there is a determination of Calprotectin or Lactoferrin makes sense in the chair. These two markers are Inflammation parameters and correspondingly often increased in Crohn's disease. Calprotectin is a substance made from neutrophil granulocytes that is released in the intestine when there is inflammation. The advantage is a particularly high sensitivity in the case of Crohn's disease. Lactoferrin is a substance that occurs in digestive secretions, for example. An increase in the stool speaks for an intestinal inflammation.
Diagnosing Crohn's disease through an x-ray
During this diagnostic procedure, a probe is advanced through the nose and throat and into the small intestine. About the probe will water-soluble contrast agent administered. X-ray images are then made at different points in time in order to show the course of the contrast medium through the intestine as completely as possible. The bowel changes typical of Crohn's disease can thus be easily and gently presented to the patient. These include above all Passage disruptions and Bottlenecks (Stenoses) in isolated sections of the intestine. Also typical are so-called Fistulas. These are connecting ducts between individual sections of the intestine. X-rays also play a role in children with Crohn's disease. Through the Disruption of nutrient uptake there is often delayed growth in children. The bone age can be determined using an X-ray of the hand and confirm the diagnosis of Crohn's disease.
Diagnosing Crohn's disease by ultrasound
In the ultrasound examination of the abdomen, the so-called Sonography of the abdomen, there are changes typical of Crohn's disease. This procedure, which is very gentle and not stressful for the person concerned, can often make the first suspected diagnosis of Crohn's disease. In Crohn's disease, there is one edematous thickening and Swelling of the intestinal wall. In the ultrasound image one can find the so-called cockade or Target phenomenon, because the thickened intestinal sections act in cross section like the rings of a target. Often enlarged lymph nodes present in response to the inflammatory process. Sometimes the fistula ducts or possible accumulations of pus (abscesses) can also be shown sonographically. If Crohn's disease has already been diagnosed, ultrasound is the simplest non-invasive examination method to check the success of the therapy.
Diagnosis of Crohn's disease by an MRI according to Sellink
The purpose of this procedure is to see the pattern and extent of bowel inflammation. The assessment of the small intestine is particularly easy with this method. Contrast media is first brought into the small intestine via a probe. This spreads over the intestinal mucosa in such a way that an optimal assessment is possible. To prevent the opposite intestinal walls from sticking together, an additional liquid is administered via the probe. The entire gastrointestinal tract can be visualized with special attention to the small intestine. An edematous thickening of the intestinal wall is typical of Crohn's disease.
Diagnosing Crohn's disease with the help of a colonoscopy and biopsy
At a Colonoscopy gets over the anus Camera hose (Endoscope) in the large intestine up to the Bauhinschen valve. This represents the transition to the last section of the small intestine. Exactly this last section of the small intestine, the so-called terminal ileum, is most commonly affected by inflammatory changes in Crohn's disease.
The pattern of involvement in Crohn's disease is always segmental-discontinuousi.e. In addition to diseased sections, there is also always healthy intestinal mucosa. In the early phase of the disease, superficial injuries to the mucous membrane, e.g. recognize reddish spots.
More constrictions occur in the later stages. During an acute attack, deeper injuries such as Ulcers (Ulcers) and Fistulas. This is characteristic of Crohn's disease Cobblestone phenomenon. This describes the changing appearance of thickening of the mucous membrane and deep ulcers. The ulcers can look elongated, like snail trails. Another pathognomonic picture typical of Chron's disease is the garden hose. Due to tissue change (Fibrosis) the bottlenecks this phenomenon occurs.
When sections of intestine stick together, one comes into being Conglomerate tumorwhich is partly palpable from the outside. During the colonoscopy, tissue samples (biopsies) are taken. In Crohn's disease, these show a multitude of immune cells, e.g. Lymphocytes, granulocytes and histiocytes. So-called granulomas are also a typical finding. Since Crohn's disease can affect all mucous membranes from the anus to the mouth, a gastroscopy is often recommended
More about Crohn's disease
- Crohn's disease
- These are the causes of Crohn's disease
- This is how Crohn's disease is treated
- Proper nutrition for Crohn's disease
- Is Crohn's disease curable?
- What is life expectancy in Crohn's disease
- Chron disease - relapse
- Chron disease and alcohol consumption, is that possible?











.jpg)