Gallstones
Synonyms in a broader sense
Medical: Cholelithiasis
Gallstone disease, Cholelith, cholecystolithiasis, Inflammation of the gallbladder, Bile, liver
English.: biliary calculus, biliary stone, cholelite, gallstone
definition
Gallstones are deposits (Concretions) in the gallbladder (cholecystolithiasis) or bile ducts (choleangiolithiasis). The formation of these gallstones is based on a change in the composition of the bile.

There are 2 main forms of gallstones:
- stones containing cholesterol (approx. 90%)
- stones containing bilirubin (approx. 10%)
Cholesterol and bilirubin are both substances that are excreted in the bile. If these are too large in the bile, they fall out (Crystallization) and form stones.
Bile ducts lead from the gallbladder and liver to the small intestine, where the bile can perform its intended function in the digestive chain.

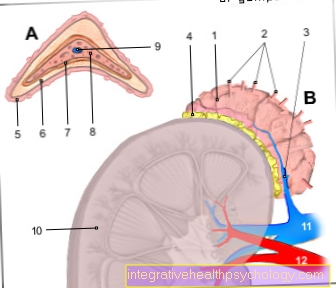
Anatomy of the liver and gallbladder
- right lobe of the liver
- left lobe of the liver
- Gallbladder
causes
The causes of gallstone disease include:
- Overweight (obesity)
- high fat diet
- pronounced weight loss and
- parenteral nutrition (Diet over a Gastric tube).
The increased incidence of diabetes mellitus (diabetes) is due to obesity (overweight) and high triglyceride levels (Hypertriglyceridemia = high fat levels in the blood).
Triglycerides are water-insoluble energy carriers and count among the blood lipids.
On the other hand, high blood cholesterol levels have no proven effect on the formation of gallstones.
Cholesterol stones
Formation of cholesterol stones:
Cholesterol can be excreted in the bile up to an amount of 500-600 ml bile / day, provided this can be bound by sufficient bile acids.
However, if the bile is oversaturated with cholesterol (too much cholesterol in the bile) and this lingers longer than usual in the gallbladder, this leads to crystallization.
Oversaturation can have the following causes:
- increased secretion of cholesterol in the bile
- decreased bile acid secretion in the bile
Pigment stones
Formation of pigment stones:
Pigment stones are bilirubin-containing Gallstones. Bilirubin is created either by an increased breakdown of red blood cells (Hemolysis) or through bacterial degradation, for example in chronic infections of the biliary tract.
In both cases there is an increased amount of bilirubin in the bile, which leads to the formation of stones.
Risk factors
The following factors increase the likelihood of gallstones:
- Female gender
- Obesity
- blond = light-skinned skin type
- childbearing age
- Age> 40 years.
Symptoms / complaints

Gallstones are in most cases asymptomatic, i.e. without complaints. Symptoms usually only arise when there is an obstruction or inflammation of the biliary tract (cholecystitis). So biliary colic occurs in about a third of the cases. Biliary colic is characterized by wave-like, severe pain in the right and middle upper abdomen that often lasts for minutes to hours. The pain often radiates to the right shoulder or back.
Further symptoms / complaints can be:
- Sensation of pressure or fullness
- Nausea and vomiting
- as well as yellowing of the skin (jaundice) due to bile congestion, as a stone has blocked an exit route and the bile is now increasingly pressed into the blood.
In very general terms, a frequent familial occurrence can also be determined. It can therefore be assumed that there is a hereditary component of this suffering.
You can find more on the subject at:
- Gallstone symptoms / discomfort
- Flank pain on the right
- pain in the back
constipation
Bile ensures that dietary fats can be absorbed in the intestine. The gallbladder is used to store the bile acids produced by the liver and is emptied into the duodenum after (high-fat) meals. If the outflow of bile is obstructed, for example by a stone, the fats cannot or not completely be absorbed and remain in the stool: so-called fatty stools (Steatorrhea), which are usually much softer than normal stool and have a strong smell. This can lead to diarrhea, but the greatly increased stool volume can also cause constipation as a symptom.
fatigue
Those affected by gallstone disease often complain of unusually severe fatigue. This is due to bilirubin, a waste product that is produced when red blood cells are broken down. Bilirubin is normally excreted with the bile and, when the bile drainage is obstructed, accumulates in the bloodstream and also in the tissue. On the one hand, this causes jaundice (Jaundice), on the other hand bilirubin has an effect on the central nervous system. The influence on the brain is usually shown by the tiredness described by those affected.
itching
Gallstone disease can make the entire skin itchy. The cause is then a (partial) blockage of the bile duct by a stone, which makes it difficult or impossible for the bile to flow out (Cholestasis). The exact biochemical mechanism is still unknown. It is believed that the problem is the accumulation of bile acids and the waste product bilirubin that is caused by the obstructed drainage. These then lead to irritation of the nerve endings, which the body perceives as itching.
stomach pain
Abdominal pain is probably the most common symptom with gallstones. This may be due to a stone that has slipped into the bile duct, causing bile congestion (Cholestasis): The result is usually a sudden, colicky (regularly recurring peaks of pain) pain. Gallstones located in the gallbladder itself can also cause pain. These occur after eating, especially after high-fat meals, as this is where the gall bladder contracts to release the bile into the intestine and the stones meet with resistance. Abdominal pain with gallstones is usually felt in the upper right abdomen and often radiates to the right shoulder blade.
Gallstone pain
Gallstones become only a quarter the so-called stone carrier symptomatic, that means doing complaints. The main focus here is on pain. Many people are only then affected alert to any gallstones and had previously noticed no abnormalities with regard to the gallbladder. For one thing, then a Tension pain in the upper right quarter of the abdomen exist which by Buttons of the gallbladder below the right costal arch while inhaling provoked can be.
On the other hand, there can also be the typical gallstones there colicky pain come. These are characterized by the fact that they seizure arise, initially increase sharply and then subside again. The pain is caused by the Gallbladder muscles when the gallstones go off against you high resistance has to work because the stones are usually larger than the gallbladder outlet. The gallbladder contracts in a wave-like manner in the direction of the gallbladder duct and can cramp due to the resistance. The Pain can do it too radiate into the shoulder or back. The occurrence of colic is related to eating high-fat food and the activity of the parasympathetic nervous system. Gallstones become symptomatic and cause painso is one Therapy urgently needed.
Diagnosis of gallstones
The diagnosis of gallstones can be made by the blood laboratory, among other things. An increase in direct bilirubin in the serum can indicate an occlusion of the bile duct.
Whether the liver has also been affected can be seen from the liver values / laboratory values (e.g. GOT). In the case of liver damage, liver values are increased. Inflammation parameters (e.g. CRP) also provide information.
You might also be interested in: How can I best lower my liver values?
Ultrasound (sonography) is the fastest and most sensitive method of detecting gallstones. Here you can recognize the stones due to their lime content as white spots with a corresponding acoustic shadow.
Read more on the topic: Ultrasound of the abdomen
Detecting gallstones can be problematic.
If the gallstones have just formed, they cannot be detected using the first-choice examination method, namely ultrasound. With the typical clinical signs (colicky pain that radiates into the right shoulder, fatty stools, aversion to fatty food, jaundice) one can almost certainly assume a stone disease.
Only when the gallstones have triggered an inflammatory reaction in the walls of the gallbladder (cholecytitis) or the biliary tract (cholangitis), and the inflammatory reaction has led to calcification of the gallstone, can the gallstones also be recognized by ultrasound.
Gallstones can also be seen in an X-ray. Without the administration of contrast agent, however, only the calcareous stones can be detected. Stones that contain little lime can be seen through recesses after the administration of contrast medium.
Because of the side effects of the contrast agent, this examination is only carried out if the following method has not led to any result.
Another method of detection is endoscopic bile duct display (ERCP). To do this, an endoscope is advanced through the esophagus, stomach and duodenum to the exit point of the bile duct.
By penetrating the bile duct, stones can be detected and removed if necessary.
More about this topic can be found: Diagnosis of gallstones
Therapy of gallstones
Treatment for gallstones is only carried out if the patient has symptoms.
The following options are available for treating gallstone disease / gallstones:
- Pain relief (analgesia) in biliary colic with medication
- non-surgical gallstone removal
- Fragmentation of gallstones by shock waves
- Recurrence occurs in 50% of patients.
- Dissolution (lysis) of the stones by MTBE (endogenous ether)
- Drug dissolution of the stones (litholysis)
- Removal of the gallbladder (cholecystectomy)
- ERCP
Pain relief is provided by pain relievers (Metamizol = e.g. Novalgin ®) and / or spasmolytic drugs to resolve biliary tract cramps (Buscopan®).
The shock wave therapy tries to cause the gallstones to pass away spontaneously by fragmenting them.
As a rule, drug-based litholysis (stone dissolution) is started about 2 weeks beforehand. An increased concentration of bile acids is ensured in order to release the cholesterol from the gallstones.
MTBE (methyl tert-butyl ether) is a cholesterol-dissolving ether and is used in the form of irrigation drainage in the gall bladder. The rinsing time depends on the stone volume.
Cholecystectomy (removal of the gallbladder) is the most common form of therapy for gallstone disease. For this purpose, a laparoscopy (so-called laparoscopy) is mainly performed with an endoscope. With this minimally invasive operation, the patient's recovery is correspondingly quick.
With an ERCP, gallstones can be found and removed with the help of an endoscope.
The therapy of gallstone disease depends on the position of the stone:
- If it blocks the gallbladder exit (the most common position), it is now treated with a complete removal of the gallbladder (cholecystectomy).
The gallbladder only has storage functions that are not essential for life, which is why the body can do without it. The earlier therapeutic approach of destruction by means of sound waves (shock wave therapy) has not proven to be meaningful in the long term, as gallstones recur regularly. - If gallstones obstruct the direct canal between the liver and small intestine, another option must be considered, as the duct cannot be removed. In this case, the attempt is usually made to use an endoscope to get through the mouth via the stomach and small intestine into the bile ducts (ERCP see above) in order to be able to remove the stone on site.
Usually the stone gets stuck at the narrow point at the mouth of the bile duct in the small intestine. Since the bile duct and the excretory duct of the pancreas flow together into the duodenum, the cocktail of digestive proteins from the pancreas also builds up. This in turn can cause acute inflammation of the pancreas (pancreatitis).
You can find more on the subject at: Therapy of gallstones
You can also find homeopathic approaches to therapy at: Homeopathy for gallstones
Gallstone surgery

Surgical removal of the gallstones comes into consideration in particular if the person affected is symptomatic, i.e. is in pain. If the patient is in a stable condition, an operation can be planned or carried out immediately in an emergency. If there are no symptoms, surgery can still be considered if the stones have the following properties: there are several stones, the gallstone is particularly large so that it fills the entire gallbladder, or there is a porcelain gallbladder, which carries a certain risk of degeneration .
When removing gallstones during surgery, there are various methods to choose from, which are used depending on the patient's condition and assessment of the gallstones. On the one hand, a laparoscopic operation, i.e. using the keyhole technique, can be performed with removal of the entire gallbladder. As a rule, the instruments for the operation are inserted into the abdominal cavity via four small incisions in the abdominal wall and can thus completely remove the gallbladder despite minimal access routes. As an alternative to the access routes in classic laparoscopic surgery, the surgical instruments, the so-called trocars, can also be inserted into the abdomen via the vagina in women, which then do not leave any scars on the abdominal wall. In some cases, open surgery may be necessary for more complicated gallstones, such as those with a very large diameter. The access can be chosen either on the right costal arch or on the longitudinal center line of the abdomen. Again, the entire gallbladder including the stones is removed.
All methods have in common that they are performed under general anesthesia. If the stones are still small and are already causing symptoms in the person affected, a so-called ERCP (Endoscopic retrograde cholangiopancreatography) - Examination, during which the endoscope can also be used to reach the bile duct, by splitting the sphincter muscle of the gallbladder to catch and remove the gallstones in this way. However, the classic and most widely used operation for gallstones is still the laparoscopic operation. As with any operation, there are certain complications, such as bleeding, damage to the surrounding soft tissue, inflammation and impaired wound healing. But these are all very rare. The prognosis after the operation is good; patients usually stay in hospital for a week after the operation.
Smashing gallstones
For the treatment of symptomatic gallstones, it is possible to consider breaking them up with targeted extracorporeal shock wave therapy. For this, however, some criteria must be met so that the therapy shows its desired effect by breaking it up. On the one hand, the stones should be free of lime and should not exceed a certain volume and a number of three stones. On the other hand, after the stones have been smashed, the stone remains are transported away, which can only take place if the gallbladder has efficient peristalsis, i.e. contracts and relaxes in a wave-like manner. It should also be ensured that the gallbladder is not inflamed.
When the gallstones are smashed, a number of 2,000 to 3,000 shock waves are sent from the outside to the body within an hour, which ideally causes them to disintegrate into small individual parts. No anesthesia is required for this, at most pain therapy. Thereafter, drugs such as bile acid can be given to promote the dissolution of the gallstones. Otherwise, the shattered gallstones will naturally pass through the urinary tract with the urine. The prognosis is normally very good, with new stone formation in around 10%.
Can you dissolve gallstones?
If gallstones have been found in the gallbladder, it is possible to dissolve them with medication or with the so-called extracorporeal shock wave therapy (abbreviated: ESWT) to smash. Drug dissolution is always an option if the gallstones are very small and not calcified. Bile acids are then taken orally (= through the mouth), which creates an excess of bile acids in the body. Due to the increased excretion of bile acids, the ratio of bile acids and stone-forming cholesterol changes in favor of bile acids. This therapy has to be done for about 6 months for it to be successful. A disintegration is an option for gallstones with a maximum diameter of 3 cm. In addition, these must not be more than three pieces and the composition must be free of lime. The ESWT is always carried out in combination with the medicinal dissolution in order to also eliminate the stone debris as effectively as possible. In the case of an existing pregnancy, inflammation in the area of the gall bladder and ducts as well as blood clotting disorders, none must ESWT be performed.The risk of recurrence of the treated disease (relapse) is relatively high both with the drug dissolution of gallstones and with the fragmentation: Up to 15% of the people treated with ESWT get gallstones again within a year, with drug therapy within new stones in almost half of those treated over the next five years. Because of this, the dissolution of gallstones is now used less often than mechanical evacuation or surgical removal of the gallbladder.
Home remedies for gallstones
The best home remedy for gallstones is arguably a low-cholesterol and low-fat diet, which can prevent the formation of gallstones. Regular consumption of fruit and vegetables also contributes to prevention. An often recommended home remedy is the daily use of apple cider vinegar: Two tablespoons of vinegar are added to two glasses of water and drunk. This stimulates the flow of bile and the excess fats have less time to accumulate in the gallbladder to form stones. Pear juice, vegetable juices, and mint tea have a similar effect.
rehabilitation
Can I live without a gallbladder?
There are generally no drawbacks to gallbladder removal. One or the other food may be worse tolerated than before, so a healthy and balanced diet should be ensured.
Complications
Inflammation of the gallbladder (cholecystiasis), perforations (tear) of the gallbladder, or secondary liver changes (liver cirrhosis) can possibly occur as complications.
A possible build-up of bile can lead to increased fluid accumulation in the bile (gall bladder hydrops).
If the common duct between the gallbladder and pancreas is blocked, inflammation of the pancreas (pancreatitis) occurs.
Inflammation of the gallbladder
Gallstone disease can lead to inflammation of the gallbladder. When a small stone slips into the bile duct, the bile backs up and accumulates in the gallbladder. After a while, the gall bladder is overly filled, which can already be felt as a bulging, elastic structure in the physical examination. In this state, the gallbladder initially becomes inflamed without the intervention of bacteria, which the affected person can already perceive through pain in the right upper abdomen radiating to the area of the right shoulder blade. As the disease progresses, bacteria can then migrate from the intestines into the gallbladder and make the condition even worse. Therapy here almost always consists of mechanical removal of the gallstones with direct removal of the gallbladder. Alternatively, the stones can be removed and the gallbladder left in the body. However, the risk of suffering from gallstones again is very high. Therefore, the recommendation is usually to have the gallbladder removed promptly.
Read more on the topic: Inflammation of the gallbladder
prophylaxis
There is no actual prophylaxis against gallstone disease.
Obesity, low-fiber and high-fat diet, however, favor the occurrence of this disease.
Therefore, you should pay attention to your body weight, eat high-fiber and low-fat foods. Coffee and fried food should also be avoided in view of the risk of subsequent biliary colic.
Can you prevent gallstones?
The formation of gallstones can partly be prevented by a conscious diet. Many gallstones are so-called "cholesterol stones" and are caused by a high proportion of cholesterol in the bile. Therefore, in order to prevent gallstones, you should be careful not to eat much fat. Cholesterol and saturated fats in particular should be avoided, as gallstones are favored by consistently high blood lipid levels. Unsaturated fats such as vegetable oils or fish oil, on the other hand, contribute to a long-term reduction in blood lipids. Such prevention is an option for people who are already at high risk for gallstones. These include women, people over 40 years of age, people with a high BMI (> 30) and people with first-degree relatives who already have or have had gallstones. Since high blood lipid levels also increase the risk of many other diseases (especially vascular diseases), such a diet is also good for people for whom none of these risk factors apply.
forecast
Surgical removal of the gallbladder (cholecystectomy), apart from the general risks of anesthesia and surgery, generally involves relatively few risks.
At all nonsurgical therapies however, the rate is the Relapse (Recurrence rate) with 30 - 50% quite high.