Thigh
General
The thigh is the upper part of the leg between the hip and the knee, or between the buttocks and the lower leg. He has strong muscles, which are mainly used for locomotion and statics.
The range of motion in the hip and knee joint, on the other hand, is much less pronounced than on the upper arm.

Thigh bone (femur)
The Thighbones (Femur) is the longest Long bones of the human body.
He will turn into a
- Headboard (Head femoris), one
- Neck part (Collum femoris) and one
- body (Corpus femoris) structured.
The two epicondyles adjoin the corpus femoris laterally (epicondyle lateralis) and towards the middle (epicondylus medialis).
- The Headboard (Head femrois) provides the Epiphysis daring
- Collum and Corpus are the Diaphysis.
- The Femoral head (Head femoris) is covered by cartilage and articulated with the Acetabulum, so forms that hip joint out.
In the head there is a small band, which is called Ligamentum capitis femoris referred to as. This tape contains a small one vessel, which is responsible for supplying the femoral head. So this tape has especially in the Growth phase crucial. This importance decreases in adulthood.
To the Femoral head closes the Neck part (Collum femoris) to distal (distant from the body) at. Then the body part of the bone follows (Corpus femoris). This is elongated and is attached to the back by the Linea aspera reinforced.
These Linea aspera consists of one
- medial (Labium mediale) and one
- lateral (Labium laterale) Portion, which in each case at the two ends of the bone (cranial and caudal) diverge.
They serve as origin and approach more numerous Muscles. There are two at the border between the femoral neck and femoral body Bony prominences.
- The great greater trochanter and
- the lesser trochanter.
In between runs the Linea intertrochanterica. These bone structures also serve as the origin and attachment point for various muscles. Further away from the body (distal) the Thighbones to two other large bony prominences, the
- Medial condyle (towards the middle) and
- Lateral condyle (laterally).
On the front side is an articular surface, which in the middle area as Facies patellaris is referred to and the connection to Kneecap (patella) represents. These two condyles each have an elevation, which is called Medial epicondyle and lateralis are designated. At these are the Collateral ligaments of Knee joint attached.
Appointment with ?

I would be happy to advise you!
Who am I?
My name is I am a specialist in orthopedics and the founder of and work as an orthopedist at .
Various television programs and print media report regularly about my work. On HR television you can see me live every 6 weeks on "Hallo Hessen".
But now enough is indicated ;-)
In order to be able to treat successfully in orthopedics, a thorough examination, diagnosis and a medical history are required.
In our very economic world in particular, there is not enough time to thoroughly grasp the complex diseases of orthopedics and thus initiate targeted treatment.
I don't want to join the ranks of "quick knife pullers".
The aim of all treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You will find me:
- - orthopedic surgeons
14
You can make an appointment here.
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
For more information about myself, see - Orthopedists.
Femoral neck
The femoral neck (collum femoris) is the anatomical section of the thighbone (femur), which connects the shaft (corpus femoris) with the head area (caput femoris). A certain angle is formed between the collum and the corpus femoris (the collum-diaphyseal angle), which should be between 125 and 135 degrees.
On the one hand, the thigh neck is exposed to great forces (transfer of force from the trunk and the upper extremity to the lower extremity), on the other hand, the thigh neck represents an additional anatomical weak point. This is why the femoral neck area is often too traumatic (due to inadequate force) or fractures of the femoral neck caused by osteoporosis (especially when older people fall). Depending on the genesis, these are usually treated with plates and letters or directly as an endoprosthesis.
Also read the article on the topic: Femoral neck fracture
Thigh muscles
The muscles of the Thigh are divided into three functional groups:
- The Extensor muscles (Extensors),
- the Flexor muscles (Flexors) and
- the muscles leading to the body (Adductors).
The group of Extensor muscles (Extensors) includes the
- Sartorius muscle, the
- Quadriceps femoris muscle and the
- Articularis genus muscle.
The sartorius muscle is the longest muscle in the human body and a two-jointed muscle, which means it covers Hip- and Knee joint. It has its origin in the anterior superior iliac spine Ilium (Os ilium) and continues on the medial surface of the Tibia (Tibia) below the head of the tibia. Because of its course, it acts as a Flexor (Flexion), weaker External rotator (Rotation in the hip joint outwards) and moves the leg laterally away from the body (Abductor). In the knee joint it leads to diffraction and Internal rotation.
The Quadriceps femoris muscle is one of the biggest Muscles of the human body and consists of four parts. All four parts have different origins, but are based on the Tibial tuberosity (Protruding bone of the tibia). The four parts are as follows:
- The Rectus femoris muscle arises from the anterior inferior iliac spine of the iliac and bends the hip joint. In addition stretches he the knee joint.
- The Vastus medialis muscle arises at the back of the thigh bone, the linea aspera, and stretches the knee.
- The Vastus intermedius muscle has its origin broadly on the front of the thigh bone and also leads to Knee extension.
- The Vastus lateralis muscle arises from the lateral portion of the Linea aspera on the back surface of the femur. It takes up most of the quadriceps femoris muscle and stretches also the knee joint.
- The Articularis genus muscle is small and a splitting off of the vastus intermedius muscle (quadriceps femoris muscle). It arises on the front of the thigh bone distant from the body and attaches to the knee joint capsule. This he tensions, so as to pinch the capsule to avoid when stretching the knee joint.
The Anterior Muscles of the Thigh (Adductors) can be divided into three layers.
- The superficial,
- middle and
- depth Adductor group.
All muscles in this group serve to bring the leg closer to the body (adduction).
The superficial adductor group contains the Pectineus muscle and the Adductor longus muscle. These arise on Pubic bone and pull towards the back surface of the femur.
The Gracilis muscle is the only two-jointed muscle in the adductor group. It also arises from the pubic bone and attaches to the shin below the head of the tibia. In the hip joint it leads to diffraction and Adduction, in the knee joint to diffraction and Internal rotation.
The Adductor brevis muscle is the only muscle that middle adductor group. This also has its origin on the pubic bone and starts on the back surface of the thigh bone.
The deep adductor group is made up of the
- huge (magnus) and
- small (minimus) adductor muscle together.
The Adductor magnus muscle arises on the ischium and attaches to the back of the thigh bone. Another part is attached to the medial epicondyle. He is considered the strongest adductor the entire adductor group.Adductor minimus muscle) is a splitting off of the large muscle and therefore has the same approach and origin.
The Flexor (Flexors) of the thigh are also called hamstring muscles designated. With the exception of the biceps femoris muscle, all muscles in this group originate at the Sciatic tuberosity (Protruding bone of the ischium) and attach to the lower leg bones. The innervation of this muscle group takes place via the Sciatic nerve.
The Biceps femoris muscle consists of two muscle heads, the
- long caput longum and the
- short caput breve.
The Caput longum also arises on the ischiadic tuberosity, while the short portion on the back of the Thighbone (Linea aspera) arises. Both muscle heads put on the head of the Fibula (Fibula) and cause flexion and external rotation in the knee joint. Since the long muscle head also pulls over the hip joint, it also leads to the Elongation and External rotation in the hip joint.
The Musculus semitendinosus sets together with the Gracilis muscle and sartorius at the center lying (medial) Shin border below the head of the shin. He stretches the hip joint and brings it to the body. The knee joint is flexed. He becomes through the Tibial nerve innervated.
The Semimembranosus muscle is flat and elongated. It lies under the semitendinosus muscle and serves as a species bearings. Its insertion is the medial condyle of the tibia. Its function and innervation correspond to that of the semitendinosus muscle.
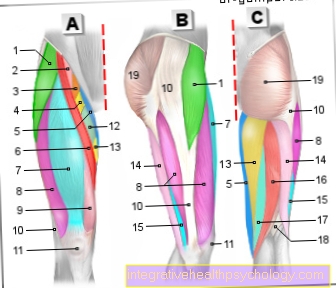
Thigh muscles
- Thigh Tie Tensioner -
Muscle tensor fasciae latae - Iliac muscle -
Iliacus muscle - Lumbar muscle -
Psoas major muscle - Comb muscle - M. pectineus
- Lean Muscle - M. gracilis
- Tailor Muscle - M. sartorius
- Upper thigh muscle -
Rectus femoris muscle - Outer thigh muscle -
Vastus lateralis muscle - Inner thigh muscle -
Vastus medialis muscle - Iliac-tibial tendon -
Iliotibial band - Kneecap - patella
- Long Dresser -
Adductor longus muscle - Big Dresser -
Adductor magnus muscle - Biceps thigh muscle,
long head -
Biceps femoris muscle,
Caput longum - Biceps thigh muscle,
short head -
Biceps femoris muscle,
Caput breve - Half-tendon muscle -
Semitendinosus muscle - Semi-membranous muscle -
Semimembranosus muscle - Femur -
Femur - Gluteus Muscle -
Gluteus maximus muscle
You can find an overview of all Dr-Gumpert images at: medical illustrations
Joints
The hip joint is the connection between the thigh and the hip (Articulatio coxae). It is a nut joint, a special form of the ball joint. The joint head lies well over halfway in the joint socket.
The joint socket (Acetabulum) is formed by the pelvis, the joint head is the head of the thigh bone (Head femoris). The hip can be in this joint
- bent (Flexion) and
- slightly stretched (Extension) become. Furthermore, the thigh can be in the hip joint
- introduced (Adduction) or
- led away (Abduction) become.
- Slight turning movements inwards and outwards are also possible.
The joint between the thigh and lower leg (knee joint) is a bicondylar joint. This means that the articular surface is formed by two condyles of the thigh (medial and lateral) and the two condyles of the tibia are formed. In this joint you can
- Diffraction (Flexion),
- Elongation (Extension), as
- Turning movements (Internal and external rotation) are executed.
More information on this topic:
- Knee joint
- hip joint
Vessels of the thigh
The great abdominal aorta (Abdominal aorta) divides in the pelvis into the right and left common pelvic arteries (Right common iliac artery and sinistra).
These in turn fork into one each
- outer (externa) and a
- inner (interna) Pelvic artery.
The vessels of the internal iliac artery supply the buttocks and thighs. The large femoral artery (arteria femoralis) emerges from the external iliac artery. This branches out into numerous smaller and larger branches and supplies both the deep and the superficial areas of the leg. In addition, branches pull towards the genital region.
The venous system is divided into superficial and deep veins. The deep large veins run roughly parallel to the corresponding arteries and have the same names. The largest superficial vein is the great saphenous vein. This takes the blood from numerous other superficial veins and ultimately guides it in the area of the groin into the deep femoral vein. All other superficial veins are also connected to the deep veins via smaller bridge veins and thus direct the blood from the periphery back to the trunk of the body.
Nerves on the thigh
The nerve innervation of the thigh takes place via the various nerves from the nerve plexus of the pelvic area (Lumbosacral plexus).
The genitofemoral nerve arises from the lumbar plexus, which sensitively affects the scrotum (scrotum) and a small part is innervated on the inside of the thigh. In addition, the femoral nerve arises from the lumbar plexus. It innervates some muscles of the thigh, including the quadriceps femoris muscle. The obturator nerve innervates the adductor group of the thigh and sensitively supplies the middle third of the medial thigh.
From the sacral plexus emerges, among other things, the posterior cutaneous femoral nerve. This is a purely sensitive nerve that innervates the skin on the back of the thigh.
The sciatic nerve is the strongest peripheral nerve in humans. It divides into two main branches, the
- Tibial nerve and the
- Common fibular nerve.
The sciatic nerve provides motor innervation to the biceps femoris muscle and then divides into its two main branches in the hollow of the knee.
The tibial nerve supplies the motor
- Biceps femoris muscle, den
- Semitendinosus muscle and the
- Semimembranosus muscle.
Then it runs centrally to the hollow of the knee and supplies various muscles of the lower leg.
Thigh pain
From an anatomical point of view, thigh pain can be divided into different groups. On the one hand, this can be muscle pain, nerve-related pain, pain due to an inadequate blood supply through the vessels or pain emanating from the thigh bone. Muscular pain in the thigh is predestined to occur after certain physical activity. A typical injury in soccer is, for example, a muscle strain in the adductor area due to the dynamic lateral movements. In general, muscular pain can result in tension, overstrain, and trauma.
Muscular complaints in the thigh area can also be caused by malpositions (congenital or acquired) (e.g. hip dysplasia). Tendon ruptures (e.g. patellar tendon as insertion of the quadriceps femoris muscle) are also possible. Nerve compression (e.g. the sciatic nerve in the buttock area) can lead to sensory and motor failures in addition to sensory disorders and pain in the thigh area.
Pain can also arise if there is too long an undersupply of blood in the thigh. This can occur, for example, in the context of a PAD (peripheral arterial occlusive disease) or in the case of a complete stenosis of the abdominal aorta in the division area of the two iliac arteries. Very often, however, pain in the thigh arises from the bone and cartilage apparatus. The femoral neck is particularly prone to fractures.
However, fractures also often occur in the supracondylar area and in the area of the femoral shaft. Due to the increasing life expectancy of people, degenerative processes on bones and cartilage, especially on stressed parts of the body, are coming to the fore. The main focus here is on osteoporotic bone changes in addition to degenerative cartilage changes in the joints. As part of these degenerative processes, fractures, misalignments or arthrosis of the joints can occur. Thigh pain can also be triggered by inflammation (e.g. of the muscles or the muscle tendons) or tumors.
Diseases of the thigh
Femoral neck fracture
The femoral neck fracture (also called the femoral neck fracture) is a very common fracture. It mainly affects postmenopausal women and patients suffering from osteoporosis. Anatomically, the femoral neck fracture is divided into a medial (inside the joint capsule) and a lateral (outside the joint capsule) fracture. The femoral neck fracture can also be subdivided using specific classifications (Garden and Pauwels classification), including the fracture line and the degree of dislocation of the fracture fragments.
Whether or not the femoral neck fracture is treated depends on these criteria. The medial femoral neck fractures are mostly caused by adduction trauma and are unstable. Surgical treatment is indicated here. In the case of lateral femoral neck fractures (lying outside the capsule), which are usually stable and caused by abduction trauma, can usually be treated as part of conservative treatment. In addition to the above criteria, the patient's age is also decisive for the choice of the surgical procedure.
In the case of young patients, a screw fixation that retains the femoral head is generally preferred. Due to the arterial blood supply, this should take place within the first six hours after the fracture. Elderly patients are given preference for endoprosthetics. The reasons for this are the mostly reduced bone density in older patients and the desire to achieve early mobilization. It is essential to pay attention to possible complications with femoral neck fractures. As with all fractures, this is a possible bleeding or thrombosis or embolism. If there is no blood supply, necrosis of the femoral head can also occur.
You might also be interested in this topic: Healing time of the femoral neck hernia
Thigh contusion
A thigh bruise is caused by a contusion of the muscular tissue caused by various causes. In addition to the muscles, the skin, fat and connective tissue are squeezed. The cause can be falls, traumatic compressions, the impact of objects, etc. Especially in the case of bruised thighs, one speaks of the typical "horse kiss".
In the case of a harmless bruise, there is initially no bleeding into the tissue or swelling. However, if the bruises are severe, these can occur. The movement of the thigh is severely restricted by the severe pain. Therefore, the PECH rule (break, ice, compression, elevation) also applies here. To treat the pain of a bruised thigh, arnica-containing ointments, Bepanthen or paracetamol can be used orally.
Thigh strain
A thigh strain is an acute clinical picture in which excessive overstretching of the muscles in the thigh leads to stabbing pain. The thigh strain is one of the typical sports injuries. Basically, this is a more harmless injury than a ruptured muscle fiber. The thigh strain is pathophysiologically based on a destruction of the microstructure of the muscle (sarcomere).
It is important to know that strains of the muscles occur in a few cases without impairing the muscle structure beforehand. For example, if there is a specific joint deformity or pre-existing muscular damage, a strain is favored. However, constant overloading of the muscles increases the likelihood of a strain occurring. Sports with typical jerky dynamic movements combined with many changes of direction are typical for the occurrence of thigh strains (e.g. football, tennis, basketball, squash, badminton).
The continuous intake of anabolic hormones or steroids also favors the occurrence of muscle strains, since the muscles here grow beyond the physiological level. With proper treatment of a thigh strain, this is an injury with a good tendency to heal. Important rules are immediate protection of the affected muscles combined with elevation, cooling with ice and compression with a pressure bandage. (PECH rules: break, ice, compression, elevation).
More on this: Torn hamstring on the thigh
Summary
The thigh consists of the largest tubular bone (Femur) of the human body and numerous
- Muscles,
- Vessels and
- annoy.
The muscles especially serve the Locomotion, as well as for attitude in an upright position.
They are divided into three broad groups:
- The Straightener (Extensors), the
- Flexor (Flexors) and the
- Adductors.
The thigh is connected to the trunk via the hip joint, and to the lower leg via the knee joint. Various movements are also possible in these joints, but these are much less pronounced than in the arm. The thigh is supplied with blood vessels via the main branches of the large arteries from the abdominal aorta.
The venous Reflux occurs through the deep and superficial Veinswhich are connected to each other and thus transport the blood from the periphery to the trunk of the body. The nerves of the thigh come from two large nerve plexuses: the Sacral plexus and lumbar. These give off numerous larger and smaller nerves, which innervate the muscles in a motorized manner and the skin of the thigh in a sensitive manner.