Therapy of biliary tract cancer
Synonyms in the broadest sense
Therapy of biliary tract carcinoma, biliary tract tumor, treatment of biliary tract carcinoma, cholangiocellular carcinoma (CCC), cholangiocarcinoma, biliary system cancer, Klatskin tumor, hilar cholangiocarcinoma
Note
All information given here is only of a general nature, tumor therapy always belongs in the hands of an experienced oncologist (tumor specialist)!
Note: bile duct cancer
It is a continuation of the topic of biliary tract cancer.
Staging
An exact assessment of the tumor stage is often only possible after the operation, when the tumor has been removed (resected) and the surgical specimen (resected material) and the lymph nodes have been examined finely (histologically).
1. T stages:
- T0: No evidence of the primary tumor
- Tis: Carzinoma in situ. This is an incipient tumor that has not broken through the basement membrane and therefore cannot metastasize because it has no connection to blood vessels.
- T1: tumor is limited to one bile duct
- T2: Infiltration outside the bile duct
- T3: Ingrown (infiltration) into the liver, gallbladder, pancreas and / or branches of the portal vein (Vena portae) and branches of the hepatic artery (Arteria hepatica) each from the left or right.
- T4: Tumor grows into one or more neighboring structures: main trunk of the portal vein or its branches from the right and left lobes of the liver, the hepatic artery (common hepatic artery) or neighboring organs such as the large intestine (colon), stomach, duodenum (duodenum) and Abdominal wall.
2. N stages:
- N0: No lymph node metastases detectable
- N1: Surrounding (regional) lymph node metastases between the porta hepatica and the duodenum (hepatoduodenal ligament) affected.
3. M stages:
- M0: no distant metastases detectable
- M1: distant metastases (especially liver, later also lungs)
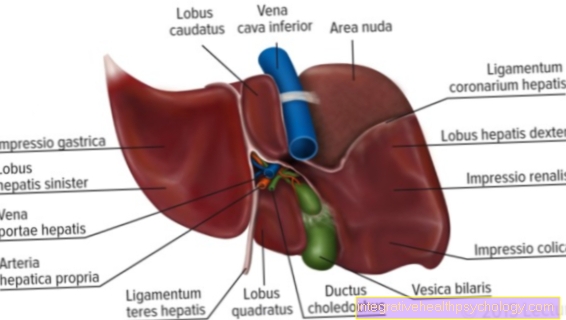
Of the Klatskin tumorwhich arises at the confluence of the biliary tract from the right and left lobes of the liver has a special division. This is also called the classification Bismuth Corlette:
Type I:
The tumor only infiltrates the common hepatic duct.
Type II:
The tumor reaches the bifurcation of the common hepatic duct
Type IIIa:
The tumor infiltrates the bile duct for the right lobe of the liver (ductus hepaticus dexter) and also reaches the associated liver segment influx
Type IIIb:
The tumor infiltrates the bile duct for the left lobe of the liver (ductus hepaticus sinister) and reaches the associated liver segment influx
Type IV:
The tumor infiltration reaches the liver segment biliary ducts on the right and left side.
therapy
The therapy of bile duct carcinoma turns out to be very difficult, since the carcinomas are often found in a non-curable (non-curative) stage. However, healing is only possible through an operation in which the entire tumor could be removed, including the affected lymph nodes. If the tumor has progressed too far and surgery is no longer possible, palliative therapy is indicated. This means that a curative approach is no longer possible and that the therapy can alleviate the symptoms caused by the tumor.
- Operational approach
Complete surgical removal of the tumor is the only curative therapy for this disease. Unfortunately, surgery with curative intent can only be attempted in 20% of those affected. As an example, patients with a Klatskin tumor of Bismuth Corlette types I and II will undergo surgery.
During the operation, in addition to the affected bile ducts, the gallbladder (Cholecystectomy), the neighboring lymph nodes, often also part of the liver (Partial liver resection) removed, as the tumor has often already grown into it. Restoring the smooth drainage of bile is important during the operation. Liver transplantation may be considered in certain patients with inoperable bile duct cancer.
- Pathological diagnostics
After removal by the pathologist, the bile duct tumor becomes fine-tissue (histologically) judged. For this purpose, the tumor specimen is cut at certain points and at the resection margins. From these samples wafer-thin sections are made, stained and under the microscope judged. The Tumor type determined, assessed its spread in the gallbladder wall and examined the removed lymph nodes for tumor involvement. It is also important that there is sufficient distance between the tumor margins and healthy tissue so that there should not be any tumor cells at the incision margin that could later cause the tumor to grow again (relapse). Only after the pathological findings can the tumor be clearly identified TNM classification, which is the primary tumor (T), the lymph nodes (N) and the distant metastases (M.) describes, are classified.
- chemotherapy
Unfortunately, biliary tumors are often not very sensitive to them Cytostatics ("cancer drugs")so that chemotherapy has little chance of success in the sense of a meaningful life extension. Numerous studies are looking for a suitable combination of cytostatics and other drugs that effectively inhibit tumor growth.
- Radiation therapy (radiotherapy)
Radiation therapy is also not very successful in bile duct cancer. In addition, the radiation sensitivity of neighboring organs (such as the small intestine, liver and kidney) must be taken into account; the radiation dose should then be selected correspondingly lower. Another option is the so-called Small area irradiation (Brachytherapy). With this therapy, a small radiation source is introduced into the immediate vicinity of the tumor with a catheter in an ERCP examination (if necessary PCT examination; see diagnosis of biliary tract cancer). This can then exert the radiation therapeutic effect on site.
You can find further information under our topic: radiotherapy
- Photodynamic Therapy
The Photodynamic Therapy (PDT) is a relatively new type of therapy. Before the actual treatment, a drug is administered via the vein (intravenously). This drug is a so-called photosensitizer, which accumulates quite selectively in the tumor tissue and makes it particularly sensitive to light. Photoactivation by means of light with a low wavelength is carried out 2 days after the drug has been administered. For an ERCP or PTC, a probe is placed in the bile duct, which emits the light. The activated photosensitizer in the tumor tissue can destroy the cells and cause the tumor to melt down. Attempts are currently being made to improve the penetration depth of the PTD.
However, PTD also has some side effects. For example it can be a Inflammation of the biliary tract come (Cholangitis). In addition, the photosensitizer can sometimes also be used to sensitize other tissues to light, so that careless exposure to the sun can cause burns to the skin can come (phototoxic skin damage).
Palliative therapy
Palliative therapy plays an important role in the treatment of bile duct cancer. Particular attention should be paid to the outflow of bile in jaundice. The ERCP is available for this. During this investigation, a Plastic tubes (Stent) is placed in the narrowed bile duct to ensure drainage again. If the bile ducts cannot be probed, the bile can be drained outwards. For this purpose, a Percutaneous transheptic drainage (PTD) placed. By eliminating the Jaundice, many symptoms are alleviated and some complications are prevented, such as hepatic coma and infection of the bile (cholangitis), thus extending survival time and maintaining quality of life. Also to consider are the Tumor painthat in the course of the disease by an experienced Pain therapists should be treated.
An important accompanying measure for all tumor patients in the late stage should be psychosocial therapy, e.g. in the form of self-help groups.