thorax
Synonyms in a broader sense
- chest
- Rib cage
- Chest cavity
- Sternum
- sternum
- Ribs
- Thoracic spine
- diaphragm
- lung
English: chest, ribcage, thorax
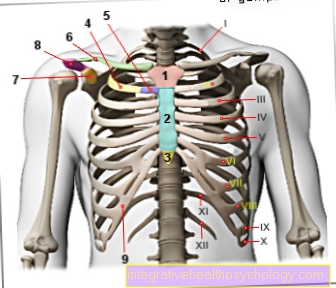
Figure thorax

I - XII ribs 1-12 -
Costa I-XII
1st - 3rd sternum -
sternum
- Sternum handle -
Manubrium sterni - Sternum body -
Corpus sterni - Sword extension -
Xiphoid process - Rib - Costa
- Costal cartilage -
Cartilago costalis - Collarbone - Clavicle
- Raven beak process -
Coracoid process - Shoulder corner - Acromion
- Costal arch -
Arcus costalis
You can find an overview of all Dr-Gumpert images at: medical illustrations
Anatomically limiting the chest (thorax) upwards and downwards in a standing person (craniocaudal direction) are two openings in the thorax, an upper thoracic aperture (superior thoracic aperture) and a lower thoracic aperture (inferior thoracic aperture).
The upper one mediates the transition from a centrally located connective tissue space in the chest (mediastinum) to the connective tissue space in the neck. As a result, in addition to numerous blood vessels, nerves and lymphatic tracts, the windpipe (trachea) and the esophagus (esophagus) in particular pass from the neck into the chest (thorax). The upper thoracic aperture is enveloped at the front by the first two ribs (Costae, Singular Costa) and a retraction of the sternum (Incisura jugulars sterni), at the back by the first thoracic vertebra (see spine, thoracic spine).
The lower thoracic aperture marks the change from the chest to the abdominal cavity and is separated from it by the diaphragm, which extends within the aperture (Latin for opening) and changes its position considerably when breathing.
Limiting the lower opening is a sword-shaped extension of the sternum (processus xiphoideus), the costal arch on each side of the body and the ends of the last two ribs (11th and 12th ribs usually end freely in the abdominal muscles and have no contact to the costal arch), behind the last, the 12th thoracic vertebra.
The boundary between the abdomen and chest, which can be assumed from the outside, does not match the actual anatomical one, for example the space under the right costal arch (Arcus costalis dexter) is almost entirely different from the liver filled in, which belongs to the right upper abdomen.
Similar to the transition from the neck to the chest At the transition from the chest to the abdomen, a large number of prominent conduction pathways (blood vessels, lymphatic systems, nerves) as well as the esophagus pass through the lower aperture and penetrate the diaphragm at certain sections. The anterior and posterior boundaries (dorsoventral direction) of the thorax in an upright person are the bony-cartilaginous elements of the ribs, the sternum and the posterior Spine, which describes an arc to the rear (breast kyphosis). These are supplemented by an elaborate system of connective tissue (bony-cartilaginous elements + ligamentous apparatus = "ligamentous thorax", passive musculoskeletal system of the chest) to form a wall for the thoracic cavity (cavitas thoracis) located inside this chest, in which the thoracic viscera also come to lie .
Let me briefly mention the joints of the thorax referenced. The thoracic spine is actually hardly bendable, only the rotation is noteworthy.
Our 12 pairs of ribs (each half of the body usually has 12 ribs, hence "pairs of ribs". Counting is from top to bottom) are in their rear origin on the thoracic spine with two "real" joints (diarthrosis) in connection with this, first of all the head of the rib (Caput costae) with a retraction at the Vertebral bodies (Corpus vertebrae) and secondly the cusp (Tuberculum costae) with the transverse processes of the whirl is articulated. These are largely uniaxial swivel joints, the axis of which runs through the neck of the ribs (Collum costae), only the ribs 6-9 form sliding joints with the transverse process of the at their cusps Vertebraso that the hump does not rotate, but rather slides slightly up and down. With the exception of the two lowest ribs, each has some kind of contact with the Sternum (Sternum), so that the ribs form a closed ring system, which results in the continuity of the thorax, e.g. the 3rd rib of the left half of the body together with the sternum and the 3rd rib of the right half of the body form a continuous arch.
On the sternum, the ribs are held in place by "fake" joints (synarthroses) that are more or less tight and hardly allow movement. The twisting of the cartilaginous part of the ribs in conjunction with the rotation they experience at the back of the spine is therefore decisive for the movement of the ribs on the sternum. In sum, this results in an upward swiveling of the ribs that widens the chest cavity during the inhalation (Inspiration), opposing movements during exhalation (expiration).
The ball-and-socket connection of the Collarbone with the Sternum rather plays with the movements of the Shoulder girdle and the poor matter. Between Ribs one half of the body remains a free space, intercostal space (Spatium intercostale). This one is with Musculature, especially the intercostal muscles (musculi intercostales) and ligaments, which, in addition to the continuity of the rib ring system in the horizontal (transversal) direction, causes tension from bottom to top (dorsocranial direction).
At the bottom and slightly inclined towards the inside of the chest, a groove (sulcus costae) is hidden on each rib, which passes through Intercostal muscles is limited. The arteries, veins and nerves (arteria, venae et nervi intercostales) which systematically supply the chest wall run in this channel.

Structure of the thorax
- liver
- diaphragm
- heart
- lung
- windpipe
- thyroid
- Collarbone
- rib
- Chest wall
- Pleura (Pleura)
- stomach
- Colon
The view of the human skeleton from the front (ventral) reveals the bony-cartilaginous components of the thorax: breastbone (sternum), ribs (costae, singular costa) and the thoracic spine.
The transition from the costal bone to the costal cartilage and the thoracic apertures can be clearly seen here.
In order to gently open up this overall structure, for example for an operation on the heart, a lot of effort and sensitivity are required on the part of the medical professional. Thoracic surgery is a demanding specialty.
The walls of the chest protect the viscera: the heart (cor), a lung (pulmo) in each half of the body and the thymus (sweetbread). In addition, there are extremely important conduction pathways, i.e. blood and lymph vessels, nerve tracts. The thorax, heart and lungs require the ability to make large changes in size while they are performing their functions; Thorax and lungs for breathing, the heart to fill with blood or to expel it.
The construct that enables this mechanism is indispensable for understanding our chest cavity and, by the way, our stomach! It is called "serosa" or "serous skins", always consists of two layers of cells (leaves) and is different in each of the organs involved named:
- Lungs: pleura, pleura
- Heart: pericardium, pericardium
- Belly: peritoneum, peritoneum
and follows a basically trivial principle: Imagine an inflated balloon, which is firmly knotted at its opening. You can bend your clenched fist into this balloon at any point until it comes to rest in the center of the balloon. One layer of the balloon wall lies directly against your fist, the other is on the outside, as in the initial state. Now push your fist forward until the two rubber layers of the balloon touch. Done! Transferred to organ systems with serous membranes, heart, lungs, abdominal cavity, the fist corresponds to the organ, your arm to the suspension of the organ, the balloon layer of the cell layer close to the organ (visceral leaf) and the cell layer on the outside of the wall-facing cell layer (parietal leaf) ).
We now apply all of the above-mentioned conditions to the thorax (rib cage): The lungs are, in analogy to the fist and the balloon, fused with the cell layer near the organ (pleura, pleura visceralis) and are only separated by a small gap (pleural gap) the wall-facing cell layer (pleura, parietal pleura), which in turn is fused with the rest of the chest wall (muscles, connective tissue, ribs, sternum, spine), in a displaceable but sticky connection.
One could only speak of a chest cavity in the sense of the word “cave” if the lungs and the organs of the mediastinum had been removed; in living humans (in situ) the entrails almost completely fill the chest. The parietal pleura (pleura parietalis) is like wallpaper for the space inside our chest, it lines it and the inner pleura (pleura visceralis) envelops the lungs (the fist from our mind game) and steps from the inside to the outer wall "Wallpaper sheet".
In addition, it must be said that from the "wallpaper" (the parietal pleura) two depressions like room dividers extend into the depth of the chest, which subdivide the space and delimit the central connective tissue space (mediastinum) of the chest from the side. The two membranes of the pleura stick together because there is a slight negative pressure in the mentioned gap (pleural gap) and it is filled with a few milliliters of "serous fluid", so that "adhesive forces" arise, comparable to two lying on top of one another damp glass panes. If the two skins lose their contact with each other, for example when a knife stabbed the chest, the affected lungs collapse due to their tendency to contract spontaneously (retraction force of the lungs), while the thorax expands as usual when breathing. In this case, the lungs cannot follow the breathing excursions of the chest; without an intact pleura, productive (sufficient) breathing is not possible.
As already mentioned, the chest expands for everyone visibly through the activity of the breathing and auxiliary breathing muscles when inhaling (inspiration) just as the stomach bulges. It is only through this increase in volume during inhalation that the interior of the lungs is enlarged to such an extent that air can flow into the lungs from the outside. The opposite happens during exhalation (exhalation), the chest and stomach flatten out. This increases the pressure inside the chest while the volume decreases, and air flows out of the lungs via the windpipe (trachea) to the outside.
In other words: only because the lungs are connected to the wall of our chest through the two layers of the pleura (pleura) can we breathe. Now we have already learned about the considerable demands that our species makes on its chest cavity. On the one hand, it must have sufficient stability to protect the viscera and, on the other hand, the mobility (viscoelasticity) to ensure the respiratory function.
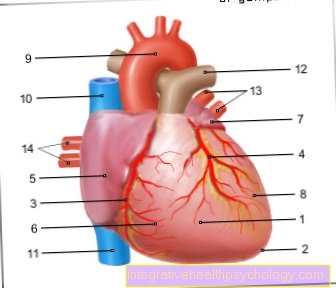
As we already know, part of the thorax / rib cage as a whole is a space of connective tissue located in the middle of the chest, the mediastinum. Towards the head it goes over into the connective tissue of the neck, below it ends at the diaphragm. Its lateral borders are formed by the wall-mounted outer pleura. Within the mediastinum, the structures outweigh each other in importance, the most decisive are: The heart (Cor) including the pericardium and the thymus (Bries), the main human artery (aorta), the superior vena cava (superior vena cava) , the pulmonary arteries and veins (Arteriae et venae pulmonales), left and right phrenic nerves (including nerve supply (innervation) diaphragm)) as well as the various divisions of vegetative nerves such as the vagus nerve or the trunk, the most powerful lymph vessel (breast duct, thoracic duct) , Esophagus (esophagus) and windpipe (trachea) or left and right main bronchus (bronchus principalis sinister et dexter).

- Collarbone
- rib
- lung
- Chest wall
- heart
- diaphragm
- liver
- Mediastinum
- Skin artery (aorta)
- Superior vena cava (Vena cava)
Anatomy and function
The terms chest or chest (thorax) represent a generic medical term both for the upper part of the trunk in its entirety and, viewed in isolation, for its bony-cartilaginous structures.
Structure of the thorax
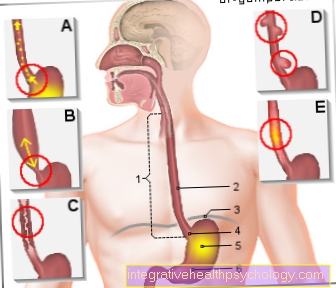
A cut has now been made parallel to the forehead (frontal cut), which even hits the intestines. Both lungs are cut, the heart, which was partially covered by the lungs, can now be seen in all its glory. In addition, the multi-storey structure of the trunk becomes clear: The abdominal cavity with the liver and stomach lies under the thorax, the diaphragm represents the border.
Diseases of the thorax
Pathological changes in the chest area can affect individual organs, for example the heart (e.g. myocardial infarction, CHD, cardiac insufficiency) as well as several structures of the ligamentous thorax at the same time and cause chest pain.
In addition, mechanical accidents in the chest area, such as after a fall, are not uncommon.
Pneumothorax
We have already mentioned a common disease, the collapse of the lungs due to the divergence of the two leaves of the pleura (pleura): the "Pneumothorax ". This occurs when air enters the pleural space and the adhesive forces of the pleura are insufficient to keep the lungs attached Rib cage to keep. In addition to accident-related (traumatic) causes, especially traffic accidents or falls, this can develop spontaneously, spontaneous pneumothorax. (especially in young men aged 15-35) when small, abnormal vesicles in the lungs (emphysema vesicles) burst. But it can also be the result of infections like the tuberculosis, degenerating fiber metabolism (Fibrosis) of the lungs or scarred remodeling of the pleura (Pleura) to be.
Further information is also available under our topic: Pneumothorax
Ultimately, there is even a genetic predisposition (disposition) due to the inactivity of certain proteins (enzymes). In addition, blood can also enter the pleura (hemothorax) or a combination of blood and air (hemopneumothorax).
Finally, the serous fluid in the pleural space can also increase (pleural effusion).
All clinical pictures have in common a shortness of breath (dyspnea) and mostly breath-dependent pain (only the parietal pleura and the rest of the abdominal wall can perceive pain) or discomfort, which is usually not particularly dangerous if only one half of the body is affected, you have two lungs , the right is more powerful. As a rule, the situation only becomes threatening when the pneumothorax is “open”, ie with damage to the body wall and a connection between the chest cavity and the outside ambient air.
In this position, which can arise after a knife stab, for example, a valve mechanism can form on the chest so that air flows in when inhaling, but cannot escape when exhaling. The pressure within the chest (intrathoracic pressure) increases accordingly, all elements of the chest are moved to the location of the lower pressure and finally press on the heartwhich can no longer develop as a result (cardiac tamponade).
The consequence would be an acute danger to life due to circulatory failure, the unavoidable therapy is a “relief puncture” through the abdominal wall so that the excess pressure can get out.
Broken rib
A single fracture of the rib is usually not a problem for the well-tensed chest wall, as long as the rib does not penetrate into the surrounding tissue, e.g. the pleura (!!). If more than three ribs are broken (series of ribs fractures) breathing is noticeably impaired and the risk of internal injury increases.
Further information is also available under our topic: Broken rib. If the symptoms are similar, however, it may only be one Bruised ribs act that is similarly painful but usually does not have such fatal consequences for the internal organs.
The continuous anatomy in the area of the upper thoracic aperture gives inflammatory processes in the head / neck area the possibility of penetrating relatively unhindered as a "subsidence abscess" into the Mediastinum to spread and cause damage there.
The basic shape of the chest wall is subject to various factors, but above all the constitution, gender and age. In women, the amount of fat storage in their "breast" in the narrower sense (mamma) dominates the contour, whereby this fat is more or less firmly suspended from a tight covering of the body, the large body wall fascia (here: fascia pectoralis), by means of connective tissue .
In men, the shape of the large pectoral muscle (pectoralis major muscle) primarily determines the shape of the chest wall.
The thorax of a person with a tendency to overweight with a short neck and strong contours (pycnics) is more barrel-shaped, in the case of a slim person with long spindle-shaped extremities (leptosome) it is narrow and flat.
Normally, when we inhale, our 12 pairs of ribs pivot upwards and the lower transverse-oval thoracic aperture widens. In old age, calcium is deposited in the cartilage tissue of the thorax (ribs have only cartilage and no bone as in the back, from about the middle of the collarbone, the "medioclavicular line", so that its mobility (viscoelasticity) decreases, it "goes." one often runs out of breath ”.
See also: Chest contusion
Emphysema
The lungs mediate the import of oxygen and the export of carbon dioxide in relation to the whole organism, which is called "gas exchange". The places of gas exchange are millions of tiny air sacs (alveoli). These can be damaged by a variety of diseases, and a Emphysema, the affected person becomes emphysematics. Difficult breathing in these patients causes the ribs to remain in an almost permanent inhalation position (swiveled upwards) with the lower thoracic aperture enlarged. Over time, this leads to one Barrel thorax while increasing the curvature of the Thoracic spine backwards (breast kyphosis).
Funnel chest / keel chest
A congenital defect of the thorax is the Funnel chest: sternum and Costal cartilage form a hollow towards the inside. Conversely, there is a clinical picture Keel breastwhen the sternum protrudes forward.
How is the thorax diagnosed?
Chest x-ray
A chest x-ray is also known as a chest x-ray. It is used to assess the structures and organs that are located in the chest area and thus enables some diseases to be diagnosed. In a chest x-ray, the radiologist can assess the lungs, the size of the heart, the pleura, the diaphragm, and the middle layer (mediastinum). In addition, particularly bony structures are easy to see on X-rays. Therefore, the chest X-ray is also used to assess the ribs, the collarbone, the sternum (sternum) and the thoracic spine.
Read more on the topic: Chest x-ray (chest x-ray)
Since the X-ray is associated with a certain radiation exposure for the patient, it is only used to rule out certain clinical pictures. These include pneumonia, pneumothorax (collapsed lungs due to air that has penetrated the space between the pleura and pulmonary membrane), pleural effusion (accumulation of fluid between the pleura and lung), hemothorax (accumulation of blood), and chylothorax (accumulation of lymph fluid) as well as emphysema (overinflation of the lungs). In addition, pathological changes can be detected in the chest X-ray, for example lung tumors, changes in the esophagus, changes in the main artery (aorta), heart diseases or diseases of the trachea.
When recording the X-ray image, there are different beam paths that can be selected depending on the indication of the recording. On the one hand there is the so-called p-a projection (posterior-anterior projection). The patient's chest is irradiated from behind while the detector plate is in front of the patient. This is the most common beam path used on patients who can stand. In addition, a side view is usually taken so that the chest can be assessed directly in several planes.
As an alternative to the p-a recording, there is the a-p recording (anterior-posterior projection), in which the patient is irradiated from the front and the detector is located behind the chest. This method is mainly used with bedridden patients. This beam path results in an enlargement of the organs in the front of the thorax in the image, since they are closer to the radiation source. Ultimately, this must be taken into account when evaluating the X-ray image. For some patients, however, there is no other option (e.g. in the intensive care unit) because the patient cannot stand up.
The recordings are usually made with the so-called hard blasting technique. X-rays with an intensity of 100-150kV are used.
CT chest
A CT of the thorax (Computed Tomography) offers an even more detailed view of the rib cage and the organs and structures in it. While the chest x-ray only provides a two-dimensional view in two planes, the CT images can also be combined to form three-dimensional images. To do this, the patient is pushed through a kind of tube on a couch, which, after emitting X-rays, detects and calculates the rays weakened by the body. The more radiation a piece of tissue lets through, the darker it will ultimately be shown on the images calculated by the computer.
It is important that the patient does not move as much as possible, otherwise blurry images can result. Ultimately arise in this way many individual sectional imageswhich are then put together to form an overall picture. The organs and structures of the thorax are displayed without overlapping and can be assessed for changes. A CT of the chest can be particularly useful for determining the exact location of a lung tumor. Even when detecting a Pulmonary embolism it is used with pleasure. Of course, the same structures are visible in the chest CT as in the chest X-ray. It is therefore suitable for assessing the esophagus, the heart, the mediastinum and the bony chest. Additionally are in the CT too Lymph nodes clearly visible. This is particularly important in the case of malignant diseases.
The reason why the CT is not routinely used instead of the X-ray is the significantly higher radiation exposure for the patient. For this reason, the CT is only requested if conventional methods such as chest x-ray or ultrasound (sonography) cannot provide sufficient information about the patient's disease. In order to obtain better contrasted images, the patient can be given a contrast medium before the examination. Since this accumulates differently in the various organs, the structures can be separated from one another even better in this way. A CT scan usually takes between 5 to 20 minutes.
Chest drain
A tube system that is connected to special bottles with or without a suction function is called a thoracic drainage. The chest drain is required to relieve the chest when air has entered the gap between the pleura and pleura. This clinical picture is known as pneumothorax. The air that has entered causes the normally existing vacuum in the pleural space to be released, so that the lungs on the affected side collapse. The vacuum is essential for the proper development of the lungs, which is why the air must be evacuated and the vacuum restored.
This is especially true for the so-called tension pneumothorax, in which more and more air penetrates the pleural space but can no longer escape due to a valve mechanism. After some time, this leads to complete compression of the lungs on the corresponding side and, as a result, to the displacement of the mediastinum with the heart, esophagus and trachea to the opposite side. This can become life-threatening within a very short time.
The drainage tube is usually inserted into the pleural space through a small incision in the skin. The localization usually corresponds to either the so-called Monaldi position in the second to third intercostal space approximately at the level of the middle of the clavicle (medioclavicular) or the so-called Bülau position in the third to fifth intercostal space at the level of the anterior axillary fold. Depending on the drainage system, a vacuum is now generated by a pump that draws the air out of the pleural space and allows the lungs to expand again. Accumulations of fluid can also be sucked off through the chest drain. Accordingly, it can be used not only to relieve a pneumothorax, but also for pleural effusions, as well as accumulations of blood and lymph fluid (haemato- and chylothorax) in the pleural space.