Basalioma of the eye
introduction
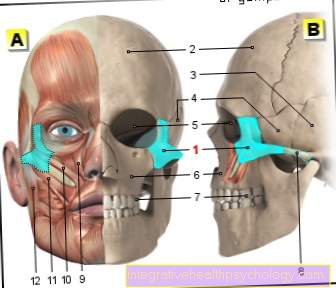
Basaliomas are malignant ulcers that affect the basal cell layer of the skin and can in principle grow on any part of the skin on the human body. In most cases, areas of the skin that are frequently exposed to the sun and thus UV light are affected. This also led to the assumption that one of the factors causing this type of skin cancer must be UV light. In most cases, areas of the skin exposed to light are often affected. In a large number of cases, these are skin areas on the forehead, temples, head and nose. Since the eye, and especially the eyelid, is often exposed to sunlight, it can also happen that basal cells develop on the eyelid.

Basaliomas in the eye area are not uncommon. These tumors require special attention because they cannot simply be treated without harming the eye and possibly the eyesight.
However, it is precisely here that rapid action is required in order to prevent the tumor from spreading so far that it damages nerves or blood vessels in the eye or can even grow to structures of the brain, which can also lead to loss of vision.
It is precisely here that the most aggressive form of basalioma, the basalioma terebrans, is feared. Due to its fast, aggressive growth, which does not stop at cartilage, bones and muscle tissue, this can lead to blindness within a very short time.
For more information, see the main page Basalioma.
Basalioma on the eyelid
The occurrence of basaliomas in the lid region is increasing steadily. Up to 90% of malignant eyelid changes are caused by a basalioma. It mainly occurs in advanced age, but can also occur earlier in rare cases. It is important that basal cell carcinoma on the eyelid is treated. The cancer cells of the basalioma almost never spread to the rest of the body, but the tumor continues to grow and can displace or destroy structures of the eye socket or the eyeball.
The basalioma on the eyelid is located in most cases on the inner corner of the eye and most often on the lower eyelid. In the case of basaliomas on the eyelid, a distinction is also made between solid basaliomas, which are usually knotty and raised with a central crust, and sclerodermiform basaliomas, which grow in the skin level and can only be defined inconsistently.
The preferred therapy for basalioma on the eyelid is surgical removal. It is important that the basalioma is completely removed so that the basalioma does not come back. Alternatively, the basalioma on the eyelid can be irradiated. In this case, however, the tumor recurs more often (compared to surgical removal) and therapy-related side effects such as dry eyes or eyelash loss up to the possible formation of cataracts (cataracts). Alternatively, the basalioma (Cryotherapy) respectively. However, there is a longer healing time with this therapy. In addition, there is no control of the extent of the tumor or whether all cancer cells have actually frozen and thus destroyed.
Symptoms of a basalioma of the eye
The symptoms of a basalioma are imprecise and are only recognized by the person concerned at a very late stage.
The main reason is that the first skin changes triggered by a basalioma are similar to everyday skin blemishes and are often overlooked.
If the tumor grows, it forms a more classic form and corresponds roughly to a string of pearls in a loop. The skin findings are not painful and are usually noticeable for cosmetic reasons. The weight loss typical of tumors is mostly absent with basaliomas.
If the basalioma is on the eyelid, it can lead to impaired movement. Those affected can usually no longer open their eyes properly, and the eye can swell accordingly and impair their vision.
Read more on this topic at: Symptoms of a basalioma
diagnosis
With advanced Basalioma In most cases, the dermatologist's visual diagnosis is sufficient to have a corresponding suspicion.
However, only the removal of the affected skin area and the pathological examination bring safety. In order to prevent cell carryover, no biopsy is taken, but rather the entire skin area is usually removed.
Therapy of a basalioma in the eye
For the attending physician, a basalioma on or in the eye is always a challenge, as therapy is particularly difficult here. Surgical removal of a basal cell carcinoma is usually the first choice. However, especially in the eye, this is rarely possible without exposing the patient to great risk. At least the removal of the surrounding tissue, which should actually always be done to be on the safe side when removing the tumor, is rarely possible without accepting massive complications.
That is why one of the other therapy options is usually used in the case of a basalioma of the eye. If this is localized on the eyelid, the icing (Cryotherapy) determined.This procedure is comparatively gentle and shows a good success rate, at least with small, superficial basaliomas. Attempts can also be made to heal the basalioma by applying a skin cream with subsequent irradiation. This is mainly done on large areas or poorly located skin areas.
Read more on this topic at: Treatment of basalioma
OP
The operation is the therapy of first choice before x-ray irradiation, icing or drug therapy of the basalioma. This is especially true for smaller basaliomas on the eyelid. In the case of larger tumors, it must be checked whether an operation is possible, as this can lead to problems with closing the surgical wound. The operation is also known as microscopically controlled, radical excision in a healthy person. This means so much that the basalioma is cut out (Excision). The edges of the cut are examined microscopically for residual tumor cells.
If cancer cells are still found in the margins, the cut is further cut out at that point. Then another check takes place. On the one hand, this prevents too much tissue from being removed, and on the other hand, tumor recurrence rarely occurs (recurrence of the basalioma in the same place). Since a basalioma on the eyelid can lead to larger wounds, it may be necessary to cover the wound with skin grafts. If the basalioma has grown in depth, it is advisable not only to cooperate with ophthalmologists, but also with ENT and / or neurosurgeons.