Vitreous bone disease
causes

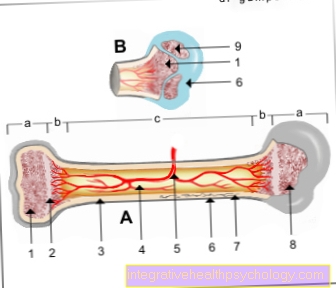
Bone is made of solid connective tissue (Collagen) that is tangled up in fibers. Calcium salts are deposited in this construct, which give the bone its final strength and mineralize it.
In the case of vitreous bone disease there is one Gene mutation on the Chromosomes 7 and 17 which contain the information for the formation of the most important collagen for bones, the Type 1 collagen. This mutation means that type 1 collagen is not formed correctly. In addition, the twisting of the individual collagen fibers is disturbed, resulting in reduced strength and stability of the bone.
General
The glass bone disease (Latin: osteogenesis imperfecta) is a disease that increases with Fragility of the bones excels. Figuratively speaking, the bones break as easily as glass, which is what gives the disease its slang name.
Glass bone disease affects around 2,500-4,500 people in Germany. That corresponds to about four to seven cases per 100,000 inhabitants.
Inheritance
Glass bone disease can be hereditary. If it has already appeared in a family, it will autosomal dominant inherited, i.e. Children of sick parents also develop this disease insofar as they receive the incorrect genetic information.
The vitreous bone disease can also spontaneousi.e. due to random mutation in the DNA arise without such a case having already occurred in the family.
Appointment with ?

I would be happy to advise you!
Who am I?
My name is I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
In order to be able to treat successfully in orthopedics, a thorough examination, diagnosis and a medical history are required.
In our very economic world in particular, there is too little time to thoroughly grasp the complex diseases of orthopedics and thus initiate targeted treatment.
I don't want to join the ranks of "quick knife pullers".
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You will find me:
- - orthopedic surgeons
14
You can make an appointment here.
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
For more information about myself, see - Orthopedists.
Symptoms
The symptoms of vitreous bone disease are primarily due to the instability of the bones.
Patients suffer bone fractures very quickly, even without external force, so-called fatigue fractures. The fractures occur more frequently by the onset of puberty and usually become less common in adulthood. Large fontanelles are often noticeable even in small children. In addition, there is often a short stature and deformities of the skeleton, e.g. scoliosis (sideways curvature of the spine) or kyphosis (hump formation).
The muscles of those affected are often below average. Other abnormalities are e.g. blue sclera (what is normally white in the eye appears bluish), hearing loss, hypermobile joints, decreased performance, increased sweating and a noticeably soft skull (rubber head).
In the context of vitreous bone disease, heart valve defects such as insufficiency (insufficient closure of the valves) or an open ventricular septum also often occur.
Classification
The vitreous bone disease can be different Subtypes are divided, each having special characteristics. The stature of those affected, as well as the severity of symptoms and the course of the disease, often differ.
Type I (type Lobstein): The type I of vitreous bone disease is this mildest Progressive form. Often it is only diagnosed when the child is older and has noticeably frequent fractures. However, it also happens that the diagnosis is made even later when accompanying symptoms become noticeable, e.g. Hearing problems in adulthood. Those affected usually have few skeletal abnormalities. Their joints are usually extremely mobile and their muscles are rather weak. The sclera may have a bluish discoloration. Otherwise type I is inconspicuous.
Type II: Type II of vitreous bone disease represents the most severe form the disease. The patients are extremely at risk of fractures and suffer from underdeveloped lungs. Previously, this form of vitreous bone disease was not considered to be viable, but now it can be treated better, which can increase survival time. Nevertheless, many children already occur during birth multiple fractures on, which is why the children often die within the first 24 hours after birth. Insufficient lung maturity is also a decisive factor in the early death of the young patients.
Type III (type Vrolik): Patients with type III vitreous bone disease also suffer from severe disease. you are short stature and have many skeletal deformities that occur on both the extremities and the spine. This can also affect breathing. Often these patients are dependent on a wheelchair.
Type IV: Type IV can be viewed as a lighter course of type III. These patients are too short stature, but suffer less from skeletal deformities and do not need a wheelchair as often as patients with type III. The sclera of those affected can be normal, but also bluish in color.
Type V: In patients with type V of vitreous bone disease occurs the phenomenon of excess Callus formation on. After fractures, excessive new bone formation occurs, resulting in thickening of the bones. In addition, calcium is deposited in these patients in the ligamentous structures between the ulna and the radius and between the tibia and fibula. This leads to problems with the In and out rotation these body parts. This can give an indication of the underlying disease during the examination.
Type VI: Patients with type VI have normal to bluish sclera. They show typical symptoms of vitreous bone disease. The peculiarity, however, is that in these patients no genetic cause for symptoms can be found. They don't have the typical gene mutations like the other patients with vitreous bone disease.
Type VII: The special feature of patients with vitreous bone disease type VII is the so-called Rhizomelia. The upper arm and thigh bones are relatively too short compared to the forearm and lower leg bones.
therapy

The therapy of vitreous bone disease is based largely on three pillars: physiotherapy, intramedullary nailing and bisphosphonates. Since the glass bone disease is genetic, it is not yet curable.
The therapy only serves to improve the symptoms.
Physiotherapy: Physiotherapy is becoming increasingly important in the treatment of vitreous bone disease. Immobility promotes the further loss of bone mass, which is why specific physiotherapeutic exercises are beneficial in order to stabilize the bones at risk of fracture. Bad posture is particularly prevented, as the muscles are built up. If possible, physiotherapy should be carried out daily. It is also a good idea to do the exercises in the water. The patients can move around easily and there is no risk of falling or fracturing.
Marrow nailing: Marrow nailing is used to directly stabilize the bones. For this purpose, the corresponding bone is divided into several pieces as part of an operation. The pieces are then threaded onto a nail or wire like a string of pearls, so that the original axis-correct position of the bone is restored. In this way, bone deformities following fractures can be avoided. Telescopic nails can also be used for this, which can be pulled apart and thus do not hinder growth. This means that the nails do not have to be changed as often due to insufficient length. However, intramedullary nailing must not be performed on patients with poor general health. It can also not be used if there is too little bone substance, as the nail does not have enough hold in the bone.
Bisphosphonates: The treatment of vitreous bone disease with bisphosphonates is a drug therapy approach.
Bisphosphonates are preparations that inhibit bone-degrading cells and thus lead to a secondary increase in bone substance. This can reduce the fracture rate in the patient. Bone pain is also less common with bisphosphonate therapy.
prophylaxis
Since the glass bone disease is genetic, it cannot get through prophylactic measures be prevented.
However, a lifestyle that is adapted to the disease can moderate its course and alleviate the symptoms. Affected people should not put additional strain on their bones, i.e. they should be on Alcohol and smoking dispense. In addition, a balanced diet that prevents overweight and underweight has a protective effect and can improve the patient's well-being.
That too physiotherapy training should be done consistently. This is how the best treatment results can be achieved.
forecast
The prognosis of vitreous bone disease depends primarily on the type of disease, i.e. on the aggressiveness of the course. This can vary greatly from patient to patient and cannot be precisely predicted. However, with today's medical measures, the overall prognosis has improved significantly.