Metastases in prostate cancer
introduction
Prostate cancer is the most common cancer in men and is the second most common cause of cancer death in men. If the cancer is at a later stage when the diagnosis is made, metastases may already have developed. Metastases are cancer cells that leave the tumor and settle elsewhere in the body. In prostate cancer, the most common site of metastasis is in the bones. The presence of metastases in prostate cancer automatically means that the tumor is assigned to stage IV and only palliative therapy options are possible.
Read more on the subject at: Prostate cancer

Where do metastases occur and why?
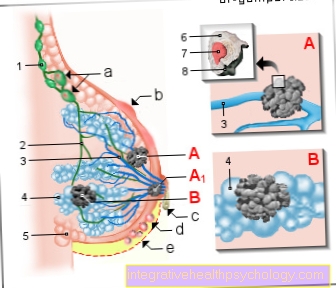
The settlement of tumor cells in other organs is called metastasis. They arise when the tumor spreads beyond its original organ and, through its growth, comes into contact with the bloodstream and the lymphatic system. The tumor cells now have the opportunity to spread to other organs via the bloodstream or the lymph, to settle here and to multiply.
A distinction is made between haematogenic (via the bloodstream) and lymphogenic (via the lymphatic drainage pathways) metastasis. Metastases in the immediate vicinity of the original tumor are called local or regional metastases. Lymph nodes near the tumor are mostly affected here. If the tumor cells settle in more distant tissues or organs, they are called distant metastases.
Read more on the subject at: Metastases
The most common sites for metastasis in prostate cancer are:
-
Lymph nodes
-
Bones especially Spine
-
liver
-
lung
-
brain
How is life expectancy affected by metastases?
In general, life expectancy is significantly shortened by the occurrence of metastases. The median survival time at diagnosis of a bone metastasis is 12 to 18 months. The five-year survival rate in the presence of metastases is only 31%.
As soon as metastases are discovered in prostate cancer, the tumor is assigned to stage IV. In stage IV, curative (healing) therapy is no longer possible and palliative (soothing) therapy is sought. The goals of this therapy are to extend the life span, improve the quality of life, slow down further growth of the tumor and alleviate the symptoms caused by the tumor itself or metastases.
Read more on the subject at: Palliative therapy
Palliative therapy for prostate cancer is made up of different pillars. The first is hormone withdrawal therapy. The tumor cells of prostate cancer grow depending on the male sex hormone testosterone. In hormone withdrawal therapy, drugs are administered that inhibit testosterone production. Thus, the tumor cells lose their greatest stimulus to growth. In addition, if the general condition is good enough, chemotherapy can also be carried out.
If there is a response to hormone treatment, life expectancy can be extended to several years.
Read more on the subject at: Hormone therapy
The other pillars of therapy are described in the sub-topics of the individual metastases. In general, however, therapy should only be initiated if these measures are expected to affect the quality of life or the lifespan. If this is not the case, the concept of “watchful waiting” can be applied. This means that those affected undergo regular examinations and the tumor and metastases are initially only observed. An advantage of this concept is that undesirable side effects of the therapy are avoided.
Bone metastases
With 50-75%, the bone is the most common metastatic site for prostate cancer. The median survival time in men with bone metastases was 21 months in recent studies. The most common areas affected by bone metastases are the spine, femur, and pelvic bones. The tumor metastasizes through the bloodstream (hematogenous) and forms osteoblastic metastases. Osteoblastic means that the bone structure is stimulated by the metastases. The bone metastases lead to severe pain and an increased risk of pathological fractures, i.e. fractures that occur without adequate trauma.
In addition to the general therapy options for metastatic prostate cancer mentioned above, there are also options that specifically affect the bone metastases and their symptoms. The most important therapy option is pain therapy. Medicines from the class of opioids are used here. In some cases, surgical stabilization of the affected bones can also lead to a reduction in pain.
Bone metastases can also be irradiated. This also leads to a reduction in pain and also has the effect that the bone becomes more stable again and breaks can be prevented. The bone can be irradiated from the outside or by means of implanted radionuclides, which emit their radiation through radioactive decay on site over a period of two to four months.
Another therapeutic option is the bisphosphonate drug group. These intervene in the bone metabolism and cells that are responsible for bone resorption. This results in more stable bone tissue and a reduction in bone fractures.
Spinal metastases
The most common type of metastasis in prostate cancer is bone metastasis. About 60% of bone metastases affect the spine and especially the lumbar spine. Spinal metastases cause pain in the back. This pulling pain is caused by the narrowing of a nerve root. Neurological symptoms up to paraplegic symptoms can also occur.
Spinal metastases are treated therapeutically like other bone metastases. This consists of irradiation either from the outside or from the inside using radionuclides. The radiation leads to the pain being reduced and the bone becoming more stable again. This can prevent broken bones. Drug therapy with bisphosphonates is also possible for spinal metastases. This group of drugs intervenes in the bone metabolism and can prevent remodeling processes in the bones and thus prevent bone fractures. The most important therapy option for spinal metastases is pain therapy. The metastases often cause very severe pain. These should be treated with opioids such as Morphine treated.
Lung metastases
Lung metastases are the second most common form of metastasis in prostate cancer, accounting for around 10%. The median survival in the presence of lung metastases is 19 months. Lung metastases usually have no early symptoms and are therefore often discovered as incidental findings in the context of imaging or during the explicit search for metastases in the context of tumor staging. If the lung metastases continue to progress and grow, symptoms such as shortness of breath, coughing up blood and pneumonia can occur.
Individual metastases can possibly be surgically removed. However, this should only be done if the operation is compatible with the general condition of the patient and a significant increase in quality of life can be expected from the operation.
Liver metastases
After bone metastases, liver metastases are the third most common metastases in prostate cancer with around 8%. Liver metastases are associated with the worst prognosis of all metastases. In more recent studies, men with liver metastases from prostate cancer have a mean survival time of 14 months.
Liver metastases are often painless and develop symptoms late. The first signs can be weight loss, loss of appetite, and weakness. If the metastases are in the center, the skin may turn yellow (Jaundice) come.
Individual liver metastases can be surgically removed. However, this operation should only be performed if there are individual metastases and the functionality of the liver can be preserved after the operation. Chemotherapy can reduce the size of the metastases. Finally, local therapy options such as laser treatments or radio frequency ablation are available. With these options, an attempt is made to locally destroy or reduce the tissue of the metastases.
Therapy for liver metastases should only be given if the treatment can achieve a significant reduction in symptoms or an improvement in the quality of life.
Lymph node metastases
Lymph node metastases are associated with the best prognosis of any metastasis in prostate cancer. The median survival time is 32 months. Lymph node metastases do not cause symptoms for a long time. They can lead to lymphedema of the legs or scrotum in later stages.
If surgery is planned, affected lymph nodes in the prostate area are removed
Brain metastases
Brain metastases can occur in prostate cancer, but are rare. If they occur, symptoms such as headache, nausea, vomiting, clouded consciousness and speech disorders can deteriorate.
Possible therapy options are surgical removal in the case of major findings or irradiation of the metastases or the entire brain. However, therapy is only recommended if it is expected to relieve symptoms or improve quality of life.
Bladder metastases
Bladder metastases are rather untypical for prostate cancer. Since the bladder is anatomically located near the prostate, if the tumor grows too much, it can spread into the bladder. The spread of the tumor into the bladder can cause urine to build up into the kidneys. The so-called urinary stasis kidneys can express themselves in the patient as flank pain and can lead to kidney weakness (Renal failure) to lead.















.jpg)