Surgery for Dupuytren's disease
Synonyms
Dupuytren's contracture; Fibromatosis of the palmar fascia, Dupuytren's disease
English: Dupuytren's contracture
Operative therapy

The medical indication for surgical treatment of Dupuytren's disease should only be made when the patient can no longer lay the hand flat on the table, i.e. when one or more fingers can no longer be fully extended (loss of extension> 20 °). If this is not the case, surgery should usually not be undertaken, as the progression of the disease cannot be predicted and the disease can, for example, stagnate over a longer period of time.
In order to be able to completely avoid surgical treatment, one should prevent Dupuytren's disease. For this, in turn, knowledge of the causes is relevant. To do this, read: Causes of Dupuytren's Disease
Apart from this, surgical therapy can also be advisable if the patient is under severe stress, for example Pain or very severe skin retraction suffers. In particular through strong skin retraction can Infections are triggered.
Operations are never risk-free. It must always be considered whether surgical therapy is advisable at this point in time. As a rule, hand surgeons recommend observing the disease for about a year first. If it is then determined that the disease is worsening and the above criteria for the surgical procedure are met, a surgical procedure can be planned.
Outpatient surgery
Is it possible to have an outpatient operation for the Dupuytren contracture?
In principle, this procedure can be carried out on an outpatient basis, but this must be decided individually. It may be necessary for patients in more advanced stages of the disease or for patients with concomitant diseases that the procedure has to be carried out in an inpatient setting. Good home care after the operation should also be guaranteed, as there are restrictions on action.
There are different ways of performing a surgical procedure. One distinguishes between:
- a fasciotomy
- a partial fasciactomy
- a total removal of the palmar fascia
- Which form of therapy is being considered varies from person to person and depends on various aspects. For example, a simple fasciotomy is usually only performed if a patient is in poor general condition or is old because of the relatively high probability of a relapse (recurrence of the clinical picture).
The surgical procedure is usually carried out as a fasciectomy. Here, the diseased fascia tissue in the palm area and the affected fingers are removed. As a rule, the diseased tissue is removed right into the healthy area in order to increase the probability that the entire diseased area was removed during the procedure. Furthermore, care must be taken during the operation that the skin supply is not damaged by injuring vascular branches.
In more advanced patients, the skin is already shortened by the changes. In such cases, skin lengthening is usually done by skin transplantation or skin plastic surgery. Under certain circumstances, it may be necessary to loosen band structures, some of which can be considerably shortened due to the curvature.
How long an operative therapy lasts cannot be answered across the board. In addition to the different surgical techniques, the individual condition of the patient is always decisive. The decisive factor here is the stage of the disease in which the respective patient is. If the disease has reached an advanced stage, fasciacotmia, as described above, can last up to four hours.
Even if a Dupuytren contracture does not require immediate surgical treatment, it is advisable not to wait until the disease is in the fourth stage. This is due to the fact that the probability of reaching a renewed full extension of the fingers involved increases if one does not wait to the utmost. Complications also occur more frequently - on the one hand during the operation, but also in the area of follow-up treatment, which can be extended in such cases.
Appointment with a hand specialist?

I would be happy to advise you!
Who am I?
My name is I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
In order to be able to treat successfully in orthopedics, a thorough examination, diagnosis and a medical history are required.
In our very economic world in particular, there is too little time to thoroughly grasp the complex diseases of orthopedics and thus initiate targeted treatment.
I don't want to join the ranks of "quick knife pullers".
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me at:
- - orthopedics
14
Directly to the online appointment arrangement
Unfortunately, appointments can only be made with private health insurers. I ask for understanding!
Further information about myself can be found at -
Forms of stunning

What forms of anesthesia are required for the procedure?
As a rule - in order to keep the risk of anesthesia as low as possible - the surgical procedure for a Dupuytren contracture takes the form of a so-called Plexus anesthesia carried out. In contrast to general anesthetic only the affected arm is anesthetized by the anesthetist applying an anesthetic in the area of the Armpit injected. About half an hour after the injection, the arm is numb so that the operation can begin.
Since the patient with a Plexus anesthesia If you are “fully” aware of the operation and not everyone would like to do so, you can also inject the patient with a sleeping pill.
It should also be mentioned positively that the patient - if their state of health allows it - can eat and drink again immediately. The Anesthesia as such is gradually disappearing. In this way, the first pain that may occur is covered by the plexus anesthesia and pain medication is rarely required.
Aftercare

In the last lines of the previous section it was already indicated that participation in the follow-up treatment plays a major role. The first follow-up treatment is started immediately after the operation. The operated hand is immobilized with a plaster splint in the first week after the operation. It is important that the fingers can move freely in all joints. A compression bandage is usually applied to the plaster splint to prevent swelling of the hand after surgery, but to allow the fingers to move.
While the sutures of the operation can be removed about 14 days after the operation, the bandages are usually only removed after the third postoperative week. Individual wound healing processes can cause the dressing to last longer.
Since every bandage should attach great importance to the mobility of the fingers, it becomes clear that the movement of the fingers will play a major role in the follow-up treatment. In consultation with the attending physician, each patient should move his fingers again without stress and as independently as possible. If patients follow the doctor's instructions and work well in this phase of treatment, no physiotherapy treatment is usually necessary.
If the swelling described above occurs in patients, lymphatic drainage can also prove to be useful.
Step by step, the hand should be brought back to the stresses of everyday life. This happens slowly and without excessive strain on the operated hand over a period of about six weeks.
Extreme loads must be avoided over a period of around 12 weeks, so that you may have to neglect your sporting activities for this period.
What else can the patient contribute to aftercare?
Rubbing the scar tissue with a fatty cream several times a day has proven itself. The scar tissue in the hand area is very sensitive and can be soothed by rubbing it in but also by lukewarm hand baths (five times a day for five minutes). Kammillosan or curd soap can be added to the lukewarm water. If you decide on both forms, it is advisable to apply the cream after the hand bath until the hand is fully mobile again.
Can the disease recur after an operation?
In general, there is a possibility of recurrence, especially in the area of the little finger (up to 50%). Relapse operations are much more difficult, so that in the event of relapse only the attending physician can advise on further therapy.
It is not possible to predict whether recurrences will occur before an operation. However, there are constellations that increase the likelihood of a relapse. If the following points apply individually or as a whole to a patient, this still does not mean that a relapse will definitely occur. It is only intended to make it clear that the likelihood of a new illness is then significantly increased.
- Dupuytren's disease runs in the family (genetic component)
- The disease has spread to other fingers (thumb and forefinger).
- Other areas of the body are affected in a similar way (see above)
- The first illness was before the age of 40.
In principle, a distinction must be made between a real new disease and a recurrence.
One speaks of a recurrence (relapse) of the disease if the same area is affected by the disease again. A new disease, on the other hand, is present if the Dupuytren contracture now relates to a different area of the hand: For example, if the little finger was treated first and now the middle finger is affected by Dupuytren's disease.
The fact that recurrences or new diseases occur is partly due to the fact that a genetic disposition is assumed. This means: Although the diseased tissue has been cleared out during the operation, it is not possible to switch off a genetic component.
Risks / Complications
Every operation involves general risks, including this one Dupuytren's disease surgery. Not least for this reason, you will be informed of the risks before the operation. In addition to the general risks, the attending physician can address individual risks that are related, for example, to your illness or other health problems.
In general, the following statement applies: There are no operation without risk!
However, complications associated with this operation are quite rare.
With every operation - no matter how small it is Infections occur. Infections can delay the healing process and may require further surgery. Medically, such an intervention is called revision surgery.
In addition, it can in exceptional cases too Wound healing disorders come, under certain circumstances the mobility of the entire hand area can deteriorate.
As part of the operation will be at Dupuytren's disease Skin grafts can be used Circulatory disorders in the skin flaps occur and thus extend the rehabilitation period. In some patients, the skin grafts may not or only partially grow into the new area.
It should also be mentioned here that most of the above-mentioned complications burden the healing time and the healing process, but the postoperative result does not have to be worsened. In most cases, however, good results are achieved.
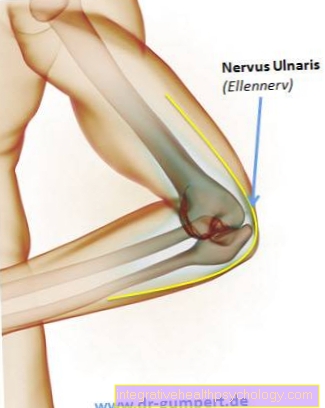
If you look at your hand, you will notice from the outside that there is “a lot in it”. So are beyond the already mentioned complication possibilities Injuries to nerves or blood vessels (larger vascular branches that supply the skin)not be ruled out. This occurs very rarely with experienced hand surgeons. In addition, there is now the possibility of reconstructing arteries or nerves through microsurgical interventions, so that postoperatively, even in this case, impairments can rarely be assumed.
Also Disturbance of the fine blood circulation are conceivable, as well as swelling in the operated area.
The attending physician will be happy to explain to you about other operational risks. Only he can assess your state of health beyond the general risks and possibly point out individual risks.
Contraindication
When should I not have an operation for Dupuytren's disease?
Individual pre-existing illnesses can prevent an operation. Depending on the general condition of the patient, the risk of an operation is too great. For example, such operations should not be planned if:
- the patient suffers from clinically evident circulatory disorders of the fingers.
- untreated eczema or already infected wound (s) are found in the area to be operated on
- the hands are already swollen preoperatively.
- The patient suffers from serious general illnesses and the risk of the operation cannot be justified (e.g. heart attack a few months ago).
It is very important for the surgical result that the patient works well and consistently in the follow-up treatment phase after the operation. If this commitment does not exist, it can also be a “contraindication”. In the next section you will see why the willingness to cooperate in the follow-up treatment phase plays such an important role.




















.jpg)



