Fecal incontinence
Synonyms
Bowel incontinence, anal incontinence
introduction
Under the term incontinence (Fecal incontinence) one understands a disease that is associated with the Inability to hold back both bowel movements and bowel movements at will, goes hand in hand.
Faecal incontinence can affect people of all ages. As a rule, however, older people are affected much more frequently.
Patients suffering from this form of incontinence experience one enormous social and psychological suffering.
Up until now it was thought that faecal incontinence is a rather rare disease that mainly affects older people, but now it is even assumed that at least 1-3 percent the population (in Germany about 800,000 people) suffer from fecal incontinence in various degrees of severity.
That lies among the people concerned Gender ratio around 1: 1.
Whereby among the men rather light forms (Stool grease) and severe types of fecal incontinence are found among women.
causes

There are a number of different causes for the development of fecal incontinence. In most cases, this type of incontinence is not caused by just one, but a combination of several factors.
The initiation of bowel movements by the organism is coordinated by various mechanisms that mesh like gears.
If just one of the underlying factors fails, this can usually be compensated for by the body's compensation strategies.
For this reason, in order to trigger fecal incontinence, there must be several irregularities that can no longer be compensated in their entirety.
The most common causes of this type of incontinence include various impulse processing disorders.
This means that the interaction between the continence apparatus and the control (or processing) at the level of the Brain no longer works properly.
Causal disorders can be caused, among other things, by a stroke, Alzheimer's disease, multiple sclerosis or Brain tumors different localization.
In addition, lead Interruptions in the transmission of impulses in many cases to the development of fecal incontinence. The information regarding the holding back and / or emptying of the intestine therefore does not find its way from the brain to the continence apparatus.
The causal problem is not in the brain itself, but at the level of the Backmarks. This problem can be triggered Paraplegia (quadriplegia), the so-called Spina bifida syndrome and the multiple sclerosis be.
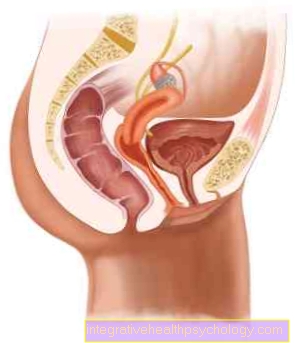
Sensory disorders in the area of the Rectum and or Rectum can provoke the development of fecal incontinence.
The underlying causes include hemorrhoids, Strength Diarrhea, a Rectal prolapse and chronic inflammation of the colon.
On the muscular level, regular stool removal can be achieved Tumors, Fistulas, Dam cracks, Abscesses and congenital malformations be hindered.
In addition, a decrease in the Pelvic floor and the overstretching of the intestine by frequent Constipation lead to fecal incontinence.
In addition to these physical causes, various medications such as Psychotropic drugs or high-dose laxatives (for example paraffins) cause fecal incontinence.
Furthermore, irregularities in the ability of stool retention are particularly common in patients with pronounced psychosis observe.
Classification and degrees of severity
Various systems exist to classify the severity of fecal incontinence. In everyday clinical practice, however, it is primarily the classification of faecal incontinence that takes place after parks Application.
This system divides faecal incontinence into three grades:
Grade 1: It is the lightest form
Intestinal winds cannot be held back and go out uncontrollably.
Grade 2: It is the medium-heavy form
Thin stools cannot be held back and come off uncontrollably.
Grade 3: It is the most severe form
Even formed chair cannot be held back.
diagnosis
The first and most important step in the diagnosis of fecal incontinence is a detailed doctor-patient discussion (anamnese).
In the course of this conversation, the patient should report on their individual symptoms.
In addition, the specialist asks about important factors such as the anamnesis during the anamnesis Stool frequency, Texture of the chair and Circumstances of involuntary defecation.
The use of medication, possible previous illnesses and / or existing allergies should also be discussed during the doctor-patient conversation.
Then the Inspection of the anal region.
The attending doctor pays attention to this irritations, Changes in the skin around the anus, Fissures, scar, hemorrhoids and Fistulas.
Then a so-called digital rectal examination carried out on the left side. During this examination, the doctor assesses both the anatomy and the function of the external sphincter. Reduced closure options can already be demonstrated at this point in the diagnosis.
In addition, manometric examinations such as the so-called Pull-through nanometry or one Measurement of the filling pressure values be performed.
In many cases, it is also advisable to carry out Procto- and Rectoscopy.
If the findings are unclear, the scope of diagnostic measures should be expanded.
The Measurement of the ability to pinch and Holding period of the external sphincter is another way of diagnosing fecal incontinence.
In addition, the so-called Electromyography the muscles as a way of delimiting a nerve damage that is the cause of incontinence.
Injuries, damage to the external sphincter or pelvic muscles can be caused by a Ultrasound examination be excluded.
Making it easier X-rays of the rectum is rarely performed.
The so-called Colon contrast enema (Contrast examination of the large intestine) the diagnosis of fecal incontinence.
All examinations to diagnose faecal incontinence are usually completely painless. However, most patients find the examination methods uncomfortable or embarrassing.
therapy

When choosing the appropriate treatment for a patient with fecal incontinence, the actual trigger a crucial role.
After an extensive diagnosis and determination of the underlying disease, a treatment plan can be drawn up together with the patient concerned.
In case of inflammatory changes in the bowel and / or the rectum, drug therapy is initiated in most cases.
Tumors can be removed during surgery.
If the cause of the fecal incontinence lies in the area of the mucous membranes or the intestinal wall, a surgical removal can also be carried out in these cases and the problem can be eliminated in this way.
The so-called "Sacral nerve stimulation“Represents a completely new method of treatment for patients suffering from faecal incontinence.
Before sacral nerve stimulation was first used in patients with fecal incontinence, it was considered a miracle cure in the treatment of urinary incontinence for years.
Basically, this procedure can be compared to how a Pacemaker be compared.
While this treatment method is being carried out, impulses from a pacemaker stimulate the nerve plexus in the area of the nerve plexus via small electrodes inserted by means of punctures Sacrum (Sacrum).
Through targeted stimulation, the external sphincter are encouraged to build up sufficient muscle strength again.
In addition, the electrical stimulation also affects the perception of intestinal contents and thus the ability to hold.
The method of sacral stimulation is particularly suitable for the treatment of neurologically caused fecal incontinence.
Forms of incontinence caused by the sinking of the Pelvic floor Can be caused by regular and targeted physiotherapy effectively treated.
Nice that pinching together several times a day of the sphincter can help increase holding power.
Drug therapy for faecal incontinence aims to prevent unexpected defecation.
With this in mind you can laxative in the form of Suppositories or Enema used to empty the bowel at a specific time.
The Adjusting the diet, for example fortifying foods with fiber, has been shown to have a positive effect on the continence system.
Furthermore, mild forms of fecal incontinence can be caused by a targeted toilet training be treated. With this method, the affected patient is supposed to learn how to clear bowel movements at a specific time each day.
In the early stages of this stool exercise, bowel movements can occur Laxative suppositories get supported. Usually a suppository is provided within the first week Bisacodyl (for example Dulcolax) is used.
If the training is successful, the active ingredient can then be used glycerin (for example Glycilax) must be switched.
After about two to three weeks When using the suppositories, a complete discharge attempt should be made.
The bowel of the patient suffering from fecal incontinence should already be able to adapt to the regular "Chair time“Got used to.
Most patients are helped during exercise by keeping a so-called stool diary in which every bowel movement is precisely recorded.
forecast
The prognosis for faecal incontinence varies considerably from patient to patient.
Both the root cause, as well as that Age of the affected patient play a crucial role in the chances of correcting the incontinence.
However, in most cases, the quality of life of the person affected can at least be significantly improved through suitable therapeutic measures.
Still, full continence (Stool control) cannot be restored in every patient.