Syphilis test
Diagnosis of syphilis

Clinically alone, i.e. based on the Syphilis symptoms, the diagnosis cannot be made because the symptoms of syphilis can vary widely and are not specific. Therefore a microscopic and serological syphilis test must be carried out. A culture of the bacteria T. pallidum on a culture medium is not possible.
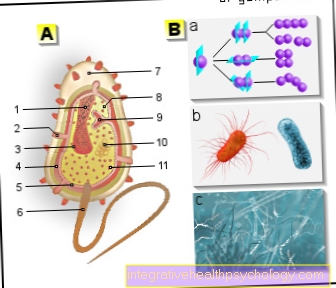
In the microscopic diagnosis of the syphilis test, a smear is taken from the skin- and changes in the mucous membrane are removed and the secretion obtained is examined under a dark field microscope. Under a normal light microscope they are bacteria not noticeable because they are too thin. In addition to the typical structure, small diameter, even turns, the rapid bending and stretching movement in the middle of the bacterium body is characteristic. A positive test - the result is proof of the disease, however, a negative result does not rule out syphilis.

In the serological diagnostics Antibody screening tests are performed that are positive 2-4 weeks after infection. Be there antibody detected that have formed against antigens that are on the surface of the pathogenic bacteria.
Of the TPHA-Test (T.pallidum Hhemagglutination test, today too TPPATest) is a sensitive and highly specific search reaction in which antibodies against T. pallidum red blood cells loaded with T. pallidum antigen (Erythrocytes) clump (agglutinate).
It becomes positive in the 2nd week after infection with syphilis and remains so for many years after the disease has healed ("Seron scar"). In the early primary stage it can still be negative. The test is used if there is any suspicion syphilis, but also for routine examinations in the Early pregnancy, from Blood donors and Blood.
Positive results require a confirmatory test: At that FTA-ABS-Test (Fluorescent Treponema Antibody Absorption Test) the bacteria are fixed on a slide and brought together with blood serum, the liquid part of the blood. The antibodies that are in the blood serum then adhere to the antigens of the bacteria. After the serum has been rinsed off, the antibodies are again labeled with other antibodies that carry a fluorescent dye. The antibodies against the bacteria are visible under the fluorescence microscope.
Of the FTA-ABS-Test is, as well as the TPPH-Test, positive in the 2nd week after infection and remains positive years after clinical healing in terms of a seron scar. Of the VDRL-Test (Venereal-D.isease-L.aboratoryTest), too Cardiolipin flocculation test called, is used for therapy and progress control.
This Syphilis test is used to detect lipid-specific antibodies that regress when the skin manifestations heal. Cardiolipin is an antigen extracted from bovine heart that cholesterol - Particle is bound. The loaded particles are brought together with the patient's serum, with flocculation in the positive case (agglutination) takes place. This test becomes positive 4–6 weeks after infection or 1–3 weeks after the occurrence of the primary effect. The amount of lipid-specific antibodies drops rapidly when the external symptoms of syphilis heal and are no longer present after successful treatment.
This quantity (titer) can be used to assess whether the therapy was successful or whether the syphilis was inadequately treated. However, the VDRL test can also be positive for other diseases, so it is characteristic, but not specific, for syphilis.
A CSF test is done to confirm neurosyphilis in patients with neurological symptoms of syphilis and to detect or rule out asymptomatic neurosyphilis. Only antibodies in the CSF that were also formed in the CNS indicate neurosyphilis, but not antibodies that have passed from the serum into the CSF. This can be determined by comparing the titre of the antibodies in the CSF and in the serum. If the ratio of CSF titer to serum titer exceeds 2, neurosyphilis is to be assumed.
Differential diagnosis of syphilis
Syphilis can manifest itself in many different ways, v. a. the symptoms of skin can be very different: “The syphilis is the monkey among skin diseases ", d. that is, it can simulate almost any skin disease. Sometimes the Roseola syphilitica Confused with drug rashes that are the result of drug intolerance. From the ulcus durum must be the painful Ulcus mollecaused by the bacterium H. ducreyi, and others caused by infections Skin changes (e.g. Granuloma venerum) are delimited.

.jpg)