Transient ischemic attack (TIA)
What is a transitory ischemic attack (TIA)?
Basically, the term TIA (transitory ischemic attack) describes a short-term circulatory disorder of the brain that presents itself in the form of neurological failures. Due to the short-term persistence of the underlying circulatory disorder, the neurological symptoms of TIA subside within a few hours.
The time it takes for these symptoms to subside is a controversial topic in medicine. Usually, however, the time window of around 24 hours is specified. The TIA occurs mainly between the ages of 60 and 70. It is believed that the cause of a TIA is the brief occlusion of blood vessels in the brain. If such a vascular occlusion persists for a long time, one speaks of a stroke. Thus, the two clinical pictures of TIA and stroke differ only in the time frame of the circulatory disorder and the resulting neurological deficits.
Also read the article on the topic: Circulatory disorder in the brain
![]()
What are the symptoms of a transitory ischemic attack?
The symptoms of a TIA only differ to a limited extent from those of a complete stroke. In most cases, however, there is no maximum manifestation of the symptoms. The symptoms of TIA are all neurological in nature. Changes in sensory perception usually occur. This can lead to significant visual disturbances, which can lead to a short-term complete loss of vision. Something similar is described for hearing. Patients with TIA often continue to experience balance disorders. The extent of this ranges from a slight dizziness to a sudden fall attack due to the loss of balance (so-called drop fit).
The language can also be significantly restricted. Here, too, the spectrum of symptoms ranges from a brief word-finding disorder to a complete loss of speech (aphasia). Depending on the affected brain area, pronounced symptoms of paralysis of the arms and / or legs can also appear. A general disorder of consciousness is almost always associated with a TIA.
In contrast to stroke, the TIA is characteristic of the fact that all of the symptoms described resolve within 24 hours and do not leave any lasting damage. Since the distinction between the two diseases can only be determined in the course of the disease, this combination of symptoms is initially always considered an emergency and is handled like a stroke.
Find out more about the topic: Signs of a stroke
This is how the transient ischemic attack is treated
Since in the acute stage of TIA no differentiation from a stroke is possible, emergency stroke therapy is always initiated first. After performing an imaging procedure, such as an MRT, to rule out bleeding, this consists of a drug dissolution of the suspected blood clot. One speaks here of a so-called "lysis" therapy.
As an alternative to this drug therapy, surgery to remove the vasoconstricting foreign body can be considered. In addition to this acute therapy, the aim of further therapy must be to prevent the further development of circulatory disorders. This also applies to a TIA, as this usually appears as a “harbinger” of an upcoming stroke and this must be prevented. The further procedure usually consists of long-term therapy with platelet aggregation inhibitors, also known as anticoagulants, such as acetylsalicylic acid (ASA) or triclopidine.
For more information, see: Stroke therapy
When will I be healthy again?
The transitory ischemic attack is by definition limited in time, which is expressed by the word “transitory”. Although there is still major controversy among experts about the exact maximum length, all symptoms must have completely subsided within a maximum of 24 hours in order to be able to speak of a TIA.
Most of the time, however, the symptoms are much shorter. In over 50%, all symptoms disappear within the first half an hour. However, when the symptoms occur, one should not wait to see whether they will go away on their own, but rather connect to a hospital as quickly as possible.
Forecast of the transitory ischemic attack
The prognosis of the transitory ischemic attack is fundamentally good, as it is by definition self-limiting and does not leave any lasting damage. Despite this, the necessary therapeutic consequences should be drawn after a TIA, even in the case of a one-off event. This is mainly due to the fact that the TIA can be a harbinger of an upcoming stroke. A third of all stroke patients had already suffered from a TIA before the event. In order to be able to assess the risk of a stroke after a TIA, doctors use the so-called ABCD2 score, which includes various risk factors for a stroke.
In order to prevent a subsequent stroke, continuous drug therapy with anticoagulants such as ASA should also be started for TIA. Should such a therapy take place, a good prognosis can generally be assumed.
Causes of the transitory ischemic attack
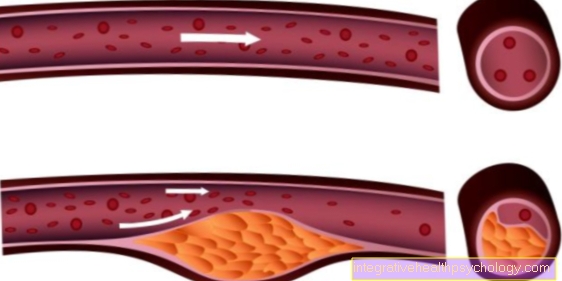
The causes of the transient ischemic attack that lead to the underlying circulatory disorder are numerous and largely similar to those of a stroke. One of the most common causes is the occlusion of a brain vessel by a vascular plug, also known as an embolus. These can arise from a wide variety of causes, such as calcification of the neck arteries or coagulation disorders, and reach the brain via the vascular system.
In addition to such an occlusion of the vessel by a foreign body, a TIA can also be caused by a migraine. This is based on a so-called vascular spasm. This causes the vessel to contract and only a small amount of blood can flow through it to supply the nerve tissue behind with oxygen. With TIA, however, despite extensive diagnostics, no triggering cause can be found.
Find out more about the topic: Blood clots in the head
Diagnosis of a transient ischemic attack
When diagnosing TIA, particular attention is paid to focal neurological deficits. Short-term circulatory disorders lead to functional failures in the affected brain regions. For example, those affected cannot move body parts for a short time or only to a limited extent. Temporary speech disorders also indicate a TIA. Since a TIA resolves after a few minutes to an hour and the symptoms completely disappear, diagnosis is often difficult.
A CT or MRI of the skull can be made to confirm the suspicion of a circulatory disorder. Early and very small vascular occlusions can be detected especially in the MRI. Since a TIA, unlike a stroke, is a short-term, usually small, occlusion, the imaging can also be inconspicuous.
With the help of an EKG, echocardiography and Doppler sonography of the cerebral arteries, possible causes of the TIA can be uncovered and the diagnosis can be made indirectly.
Do you need more information on this topic? Read our next article on this below: Cost of an MRI
How can you distinguish a TIA from a migraine?
Indeed, it is sometimes difficult to distinguish a severe migraine attack from a TIA. However, there are some indications that can point the way in the diagnosis. On the one hand, the question arises as to whether an affected person has often suffered from migraine attacks with similar symptoms in the past, since migraine attacks rarely occur again in later life.
However, the course of the onset of symptoms is particularly decisive for differentiation. Since a circulatory disorder usually occurs suddenly with TIA, the symptoms set in abruptly, only to slowly decrease again after they have reached their maximum severity. A migraine attack usually proceeds more slowly at first and the various symptoms appear slightly delayed.
Also read the article on the topic: Migraine attack
That is the difference to a stroke
The specific difference between a transitory ischemic attack and a stroke lies primarily in the duration of the circulatory disorder and thus the duration of the symptoms. The temporal difference in the circulatory disorder is probably due to the fact that TIA is mostly a matter of smaller vascular plugs that detach themselves within a few minutes and the subsequent nerve tissue can be adequately supplied with blood again. A distinction between the two clinical pictures is primarily not relevant for diagnosis and therapy, as they are each identical.
What can be the long-term consequences?
Since the TIA itself does not leave permanent damage, the greatest long-term risk in patients with a TIA is the increased risk of stroke. 30% of all those affected will suffer a stroke within the next 5 years.
In order to minimize this risk, in addition to starting anticoagulant medication, attempts should also be made to reduce other risk factors. These include above all the blood pressure and blood sugar levels in diabetics. However, the LDL cholesterol value should not exceed a certain level and a healthy lifestyle should be observed that includes a lot of exercise and little or no consumption of nicotine or alcohol. In this way, the long-term consequences of a TIA can be kept within limits, provided the risk of a stroke can be kept as low as possible.
Read more on the subject at: Prevent a stroke