U1 investigation
introduction

The child screening examinations or early diagnosis examinations U1 to U11 (also known as U-examination) have been legally introduced in Germany since 1976 and serve the purpose of prevention (Disease prevention). Behind this is the early detection of disorders of physical, mental or social development in age-dependent development phases so that these can be encouraged or treated at an early stage.
Read more on the subject at: U examinations
The examinations are carried out according to the "Children's guidelines", Which are determined by the joint federal committee. The respective findings are documented in one yellow examination book for children. The examinations have so far been offered on a voluntary basis, but there is political debate as to whether they should not be made mandatory, as neglect and violent crimes against children have become more and more common in recent years. Some federal states in Germany have already implemented this.
With the exception of U1, the early detection examinations are carried out by a pediatrician or general practitioner. Since the U1 (initial newborn examination) takes place immediately after the birth, it is carried out by the delivering Gynecologist, of the midwife or a consulted pediatrician. The pediatrician is called in above all if the birth is premature or at risk, or if complications arise.
Implementation of the U1
This examination is carried out according to the APGAR scheme, which is used to check the vital signs (breathing, heartbeat, etc.) of the newborn after birth. This checks whether the baby can stay with the mother or whether it is an emergency situation in which action must be taken quickly. In the latter case, the infant is in a very critical condition; it may have to be resuscitated and / or ventilated directly or transferred to the intensive care unit.
According to the APGAR scheme, points from 0-2 are awarded for the individual categories / letters (APGAR score).
- In this scheme, A stands for appearance and primarily assesses the skin color of the newborn. If this is pale and blue, 0 points are awarded, for rosy skin and mucous membranes 2 points. 2 points is the highest possible number of points in this score that the infant can achieve. 2 points in a category mean that everything is fine.
- The abbreviation P stands for pulse. If there is no pulse, there are 0 points, for a pulse below 100 beats per minute there is 1 point and for more than 100 beats per minute 2 points are achieved.
- The next test is that of facial movements (G). If the baby cries, everything is fine (2 points), if, on the other hand, there is no reaction, the baby is ill (0 points).
- The next step is to check whether the baby is active (A) or whether and to what extent it moves.
- The last thing to do is to check the respiration (R). The infant receives 2 points for regular breathing, which takes place approx. 40 times per minute, and no point is awarded for missing breathing.
In addition, there are other studies that aim to identify acutely dangerous malformations. If these are discovered quickly or in good time, some can prevent worse with immediate surgery. This includes probing the esophagus. You check whether there is a continuous connection between the mouth and stomach. The first signs of a lack of connection may be that the newborn does not want to drink. However, this is not a sufficient criterion, but an indication that a so-called esophageal atresia could be present.
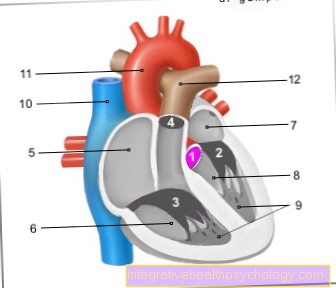
In addition to the esophagus, the nasal passages are also probed and checked for patency. Furthermore, the temperature is measured rectally (thermometer is inserted into the anus) in order to rule out rectal atresia. Rectal atresia is the absence of the lower part of the rectum and thus the lack of a connection between the intestine and the outside world.As a result, the child cannot excrete anything, which is definitely an emergency that must be dealt with immediately. Finally, the child is examined for gross deformities. These include cleft lip and palate, eye defects, neural tube defects (Central nervous system defects) such as the open back (spina bifida), Malformations of the extremities (e.g. Clubfoot or one Dislocation / dislocation of the hip), Birth injuries and water retention (Edema). Both organs are also monitored in order to detect major heart and lung disorders early on.
Read more on the topic
- Reflexes of a baby
- U2 examination
Diagnosis
This investigation is after one, five and ten minutes after giving birth carried out and the points of the individual categories added up. normal are approx. 9-10 points, at 5-8 points exists a State of depression or a slight asphyxia. Asphyxia is a threatening state of suffocation caused by the falling oxygen levels in the blood is conditional. At the same time it comes to one increasing carbon dioxide content in the blood, which makes the brain feel choked because there are certain areas in the brain stem that reduce the carbon dioxide levels in the cerebral water (Liquor) can measure.
Reaches the infant less than 5 points according to the APGAR scheme acute danger to life for the little one. For premature babies, however, the APGAR index can only be used to a limited extent because some of these children are not yet sufficiently developed for a life outside the womb and therefore require special treatment, which means that without special measures, some of them would not be viable. This index, which is designed for infants who are born regularly, is therefore not comparable for premature babies.
Possible therapeutic measures
If the infant reaches after APGAR scheme less than 5 points, it is one life threatening condition. Emergency measures such as a resuscitation and or artificial respiration initiated in order not only to save life, but also to prevent permanent damage, especially to the brain, because this organ is particularly sensitive to a lack of oxygen.
Even if there is one Esophageal or rectal atresia an emergency operation must be initiated immediately.
Cleft lip and palaten can also be corrected by an operation so that nothing can be noticed afterwards.
Vitamin K prophylaxis
An important prophylaxis is the administration of vitamin K. Every baby receives it 3 times 2 mg. This vitamin is used for that Blood clotting, i.e. clot formation, is required. The infant usually does not get enough of it because there is too little in the breast milk, the liver is not yet fully developed and the intestines are not yet colonized by bacteria that can produce vitamin K. In addition, vitamin K prophylaxis reduces the incidence of the disease Neonator hemorrhagic disease. Among them is one increased tendency of the infant to bleed to understand.