Chronic Inflammatory Bowel Disease
introduction
Chronic inflammatory bowel disease (also IBD called) are diseases of the intestine, in which there is recurrent (recurrent) or constantly active Intestinal inflammation comes.
The chronic inflammatory bowel disease often occurs for the first time at a young age (between the ages of 15 and 35) and often occurs in families.
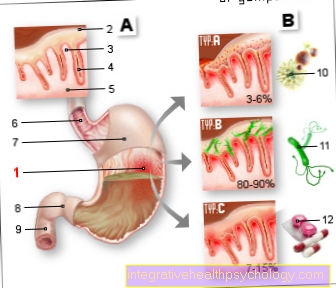
Count Crohn's disease and Ulcerative colitis one of the most common inflammatory bowel diseases. These differ in the Spread in the gastrointestinal tract and how deep the tissue is affected by the inflammation.

Thus, in Crohn's disease the entire gastrointestinal tract to be affected. The inflammation attacks all layers of the intestinal wall. In ulcerative colitis, however, is often only the colon becomes ill and the inflammation usually does not spread over the entire layers of the colon mucosa. If the distinction between the two diseases is not completely possible, this intermediate stage is called Indeterminate colitis.
Inflammatory bowel disease is caused by a excessive immune response of the body against components of the intestinal wall. The exact cause has not yet been clarified.
In addition to inflammation of the intestines can also partially Stomach and esophagus and also other organs such as biliary tract, skin, joints and eyes be affected by the inflammation.
Patients with inflammatory bowel disease typically suffer primarily from a general feeling of illness and fever severe abdominal pain and bloody diarrhea.
A treatment is definitely necessary as the inflammation causes a breakthrough of the intestine (perforation) and thus cause a life-threatening condition. The treatment takes place with Medicationthat suppress the immune system. If Complications such as suppuration, fistula formation, degeneration or narrowing of the intestinal lumen must arise operated on become. In contrast to Crohn's disease, ulcerative colitis is curable.
Because in the case of chronic inflammatory bowel disease there is an increased risk of degeneration of the intestinal cells Colon cancer is given, regular checks should be carried out by the attending physician. The Life expectancy of patients with ulcerative colitis as well as Crohn's disease is hardly or not at all restricted, provided that optimal therapy is carried out.
Symptoms
The chronic inflammatory bowel diseases ulcerative colitis and Crohn's disease differ somewhat in their symptoms. Both diseases can lead to slightly increased temperatures up to fever.
In ulcerative colitis, bloody and slimy diarrhea with a significantly increased stool frequency are the main symptom. In addition, there is often abdominal pain in the left lower abdomen and painful need to defecate (Tenesmen). Often the causes for this are flatulence.
It can also lead to extraintestinal complaints (symptoms outside the intestine).
These symptoms include primarily sclerosing cholangitis (inflammation of the biliary tract), arthritis (inflammation of the joints), skin rashes and eye infections.
Primary sclerosing cholangitis occurs in 75% of patients with ulcerative colitis.
In general, complaints outside the intestine in ulcerative colitis are rare compared to Crohn's disease.
Read more on the subject below Symptoms of ulcerative colitis
An intermittent course is typical for Crohn's disease. There is a 30% chance of getting another episode within a year. If symptoms persist for over half a year, the condition is said to be chronic.
Read more on the topic Crohn's disease attack
In contrast to ulcerative colitis, Crohn's disease tends to produce watery, bloodless diarrhea with usually only a slightly increased stool frequency.
However, constipation (constipation) can also occur.
In addition, pain in the right lower abdomen, anal fistulas, abscesses in the area of the anus and intestinal stenoses (constrictions) are to be expected as possible symptoms.
Since the chronic bowel disease Crohn's disease can occur in any section of the gastrointestinal tract, the symptoms mainly depend on the affected section of the intestine.
Since the small intestine is usually affected and this is important for the absorption of nutrients, the so-called malabsorption syndrome (impaired absorption of substrates from the intestine) and consequently deficiencies can occur. These include weight loss, anemia (anemia), steatorrhea (fatty stools), lack of fat-soluble vitamins or kidney stones.
Extraintestinal complaints also occur with Crohn's disease, which are also relatively common in this disease. Here, too, the joints are affected by arthritis (inflammation of the joints). Inflammation of the eyes (iritis, episcleritis, uveitis), inflammation of the biliary tract and skin changes occur.
Ulcers are also more common (Ulcers) and canker sores in the oral cavity.
Read more on the subject below Symptoms of Crohn's Disease
Find out more about the topic here: Burning intestines and iron deficiency and depression - what is the connection?
causes
Basically, the causes of inflammatory bowel disease are still unknown or largely unexplained.
It is assumed that it is a multifactorial event. This means that faulty genetic predisposition (Disposition) and environmental factors combine to cause inflammatory bowel disease.
The interaction of these factors appears to lead to a disruption of the intestinal barrier function. As a result, bacteria from the normal intestinal flora can get into the lining of the intestine and trigger chronic inflammation there.
As already mentioned, both Crohn's disease and ulcerative colitis primarily appear for the first time between the ages of 15 and 35 years. However, Crohn's disease can also appear for the first time in childhood, while ulcerative colitis usually only appears after puberty.
Some genes that are associated with inflammatory bowel disease have also been identified. The most important gene mutation (change in a gene) is in the so-called NOD-2 gene. The NOD-2 gene has the task of recognizing bacterial components in the intestine and then activating immune cells for defense. A NOD-2 mutation is present in over 50 percent of Crohn's disease patients.
In comparison, this gene change is rare in ulcerative colitis patients.
An important environmental factor that should be mentioned and that has different effects on the two main inflammatory bowel diseases is smoking. This means that smokers are more likely to develop Crohn's disease. In addition, smoking often makes the disease more severe, which is why Crohn's disease patients should definitely stop smoking.
On the other hand, smoking obviously has a protective effect on ulcerative colitis, since smokers tend to develop ulcerative colitis less often.
According to the latest studies, inflammatory bowel diseases are not, as assumed, autoimmune diseases.
Psychosomatic incidents, ie cause, were also excluded. However, psychological factors (such as stress) can have a bad effect on the course of inflammatory bowel disease.
Read more on this topic at:
- How to quit smoking
- Causes of Ulcerative Colitis
- Causes of Crohn's Disease
diagnosis
Stool examination
A Stool examination belongs to the standard diagnosis of inflammatory bowel disease. The stool diagnostics are mainly used to rule out bacteria caused by bacteria gastroenteritis (Abdominal influenza).
You test the stool for pathogenic (disease-causing) bacteria. In addition, the markers for a mucosal inflammation "Calprotectin" and "Lactoferrin“To be measured. These also serve to differentiate from non-inflammatory causes.
Calprotectin, for example, is a protein found in certain white blood cells (immune cells) in our body.
If these are more active, as an inflammatory process takes place in the intestine, this indicates an inflammatory bowel disease. Therefore, if calprotectin or lactoferrin exceed a certain value, this indicates an inflammatory disease.
These parameters are also used for process control certainly.
In order to differentiate between ulcerative colitis and Crohn's disease, in some cases of ulcerative colitis an increased concentration of beta-defensin-2which is only formed when there is inflammation.
In Crohn's disease patients, this value is usually low or nonexistent. However, this value may also be partially missing in ulcerative colitis patients and is therefore not suitable for reliable differentiation.
Laboratory diagnostics
In addition to clinical symptoms such as diarrhea and Pain laboratory parameters are also available to make a diagnosis.
If inflammatory bowel disease is suspected, the blood should be examined for signs of chronic inflammation, anemia, and malabsorption or malnutrition.
So definitely one should Blood count and the determination of the CRP (C-reactive protein).
A anemia and an increase in immune cells suggests chronic inflammation. In chronic inflammatory bowel disease, CRP is usually increased in the acute inflammatory flare-up, but negative CRP values do not rule out chronic bowel inflammation.
Should the suspicion of Crohn's disease harden, too should Vitamin B12 can be determined which is often lowered in Crohn's disease due to poor absorption in the lower part of the small intestine.
Furthermore, a Antibody determination often help either to identify a chronic inflammatory bowel disease or to differentiate between Crohn's disease and ulcerative colitis. These include the antibodies ASCA and ANCA. For example, the ASCA antibody occurs in 70% of Crohn's disease patients and only in 15% of ulcerative colitis patients.
therapy
The treatment of a chronic inflammatory bowel disease depends on whether an acute flare-up has to be treated or the symptom-free interval is to be extended and a new flare-up delayed.
To treat the acute inflammatory flare-up, anti-inflammatory drugs such as cortisone are mainly used.
As already mentioned, Crohn's disease patients should generally refrain from smoking, as this worsens the course of the disease. A balanced diet and adequate nutrient intake should be ensured. In addition, alcohol and certain foods that are not well tolerated should be avoided.
Read more on the subject below Diet in Crohn's disease
In the event of malabsorption, missing substrates such as vitamins, calories, protein, zinc and calcium should be substituted.
Surgical intervention can also be performed in an emergency for Crohn's disease. However, this is only the case in emergencies such as perforation (breaking through of the intestine).
Crohn's disease is mainly treated with drugs and cannot be cured by surgery.
Read more on the subject below Therapy of Crohn's disease
In the case of severe ulcerative colitis, however, the rectum (rectum) and colon (large intestine) are surgically removed, a so-called proctocolectomy. For stool elimination, either an artificial anus is created or an "ileonal pouch" is formed.
An ileonal pouch is a connection between the small intestine (Ileum) and anus and represents the standard procedure.
Since ulcerative colitis only affects the colon and rectum in most cases, it is cured by surgical removal. In the case of lighter courses, care should be taken to substitute nutrients such as iron.
Read more on the subject below
- Therapy of ulcerative colitis
- Antibody Therapy (Anka)
- Mesalazine
Medication
Drug treatment depends primarily on whether it is an acute flare-up of inflammation or a non-inflammatory interval.
The drug treatment of Crohn's disease differs from that of ulcerative colitis: In mild, acute Crohn's disease, local treatment is given with glucocorticoids such as budesonide.
Read more on this topic: Medicines for Crohn's disease
In the case of more severe attacks or if local therapy is insufficient, systemic glucocorticoid administration is carried out with e.g. Prednisolone.
If the disease cannot be controlled with glucocorticoids, the administration of immunosuppressants must be considered. TNF-alpha antibodies in particular are used here.
In order to delay the next acute inflammation as far as possible, immunosuppressants such as azathioprine or infliximab (TNF-alpha antibodies) are also given.
In the acute therapy of mild ulcerative colitis, so-called 5-ASA preparations (e.g. mesalazine), which have an anti-inflammatory effect, are used locally.
Antibiotic therapy must be given in the case of bacterial infections. Glucocorticoids are also administered for moderate attacks.
If the episode is severe, immunosuppressants such as ciclospoprin A, tacrolism, or infliximab are prescribed. For long-term therapy between attacks, the patients take 5-ASA preparations rectally or orally. Antibiotics must be used for bacterial infections.
Further information can be found here: Infliximab






.jpg)







.jpg)