ISG blocking
Synonyms in the broader sense
Sacroiliac joint hypomobility, sacro-iliac joint blockage, SIJ blockade, SIJ blockageSIG blockade, SIG blockage, sacroiliac joint blockage, sacroiliac joint blockage, sacroiliac joint blockage, sacroiliac joint blockage
definition
Under one blocking one understands a reversible deviation from the normal joint function in which the joint play (joint-play) is restricted or eliminated within the normal, physiological range of motion of a joint. A joint blockage is caused by functional or structural changes in the joint surfaces or in the soft tissue covering. One or more directions of movement of a joint or movement segment can be affected. A characteristic of the blocking is that it always has a free direction of movement.

Appointment with a back specialist?

I would be happy to advise you!
Who am I?
My name is I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
The spine is difficult to treat. On the one hand it is exposed to high mechanical loads, on the other hand it has great mobility.
The treatment of the spine (e.g. herniated disc, facet syndrome, foramen stenosis, etc.) therefore requires a lot of experience.
I focus on a wide variety of diseases of the spine.
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- - your orthopedic surgeon
14
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
Further information about myself can be found at
anatomy
The ISG (medical: Articulatio sacroiliaca) is the articulated connection between the Sacrum (Os sacrum) and the iliac bone (Os Ilium). The articular surfaces (Facies auricularis) between these two bones are boomerang-shaped to c-shaped and are located between the 1st and 3rd sacral vertebrae. They consist of an upper and lower pole, the transition point of which is approximately at the level of the 2nd sacral vertebra. There is a kink between the upper and lower pole, the angle of which is 100-120 °.
For the stability of the SI joint, the surface texture of the joint surfaces, the position of the sacrum in the Pelvic ring and a number of ribbons responsible. Because of these stabilizing factors, only small movements are possible in the ISG. Active movement in the ISG is not possible. Due to misalignments of the intestine or the sacrum, the affected ligaments are increasingly stressed. The consequence is an increase in tension in the ligaments, which can lead to a movement disorder of the SI joint and thus to a blockage.
The ISG is mainly innervated from the S1 root.
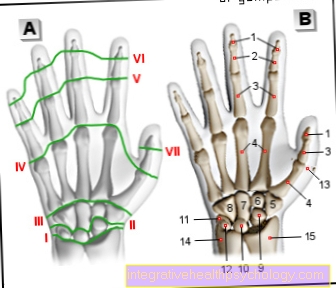
Figure ISG - blockage

ISG - blockade - conduction symptoms
- Sacrum-iliac joint
(Sacroiliac joint,
abbreviated ISG)
Articulatio sacroiliaca - Front Sacrum-iliac ligament
Lig. Sacroiliacum anterius - Iliac bone - Os ilium
- Sacrum - Sacrum
- Lumbar and sacrum kink -
Promontory - Fifth lumbar vertebra -
Vertebra lumbalis V - First lumbar vertebra -
Vertebra lumbalis I - Thoracolumbar junction
- Twelfth thoracic vertebra -
Vertebra thoracica XII - Hip joint - Articulatio coxae
Pain radiation areas:
A - lumbar spine (lumbar spine)
B - buttock region - Gluteal region
C - Groin - Inguinal region
D - front and back leg
E - knee
You can find an overview of all Dr-Gumpert images at: medical illustrations
General
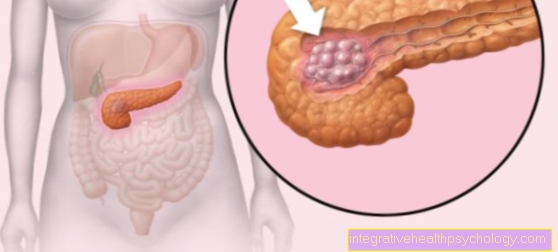
- The Sacroiliac joint is one of the most therapy-intensive areas of the body affected by pain
- 60-80% of the population suffers from an ISG blockage and therefore from once in a lifetime Back pain.
- Blockage of the SIJ can occur at any age and affects men and women equally.
- The Sacrum and iliac joint is the turning point of the uniaxial locomotor organ Spine on the biaxial locomotor organ legs. These transition zones are particularly prone to malfunctions.
- Other transition zones in which blockages often occur are the head joints, the cervicothoracic transition (transition from the cervical to the thoracic spine) and the thoracolumbar transition (transition from the thoracic to the lumbar spine).
causes
As already mentioned at the beginning, the SIJ like any other joint has a physiological joint clearance (joint-play). This is understood to be the sum of the passive movement possibilities that a joint can perform and is therefore a basic requirement for normal, healthy joint function. If this joint play is reduced, there is a blockage.
With regard to the sacroiliac joint, the cause of a blockage is usually a lifting trauma or, traditionally, stepping into space, for example when overlooking a step.
Blockage of the SI joint often occurs as an accompanying phenomenon in other orthopedic diseases, such as after hip operations or in the context of spinal diseases.
Discomfort / symptoms / pain at the SI joint

The main symptom is back pain, which is often described as deep lumbar and usually occurs on one side. Pain intensification after prolonged sitting and an improvement in symptoms through exercise and the application of heat are common.
Often there is a radiation of pain in the buttocks area, in the groin and in the lumbar spine. A combination with abnormal sensations such as tingling and pins and needles is also observed. Knee pain should also make the doctor think about the differential diagnostic possibility of an ISG block.
The symptoms of ISG blockage belong to the group of pseudoradicular pain syndromes.
Basically, radicular pain syndromes can be distinguished from pseudoradicular pain syndromes.
Pseudoradicular pain is pain that is not caused by root irritation. Traditionally, patients report back pain that radiates into the leg, can affect the front and back of the leg, but usually ends in the knee area. The back of the knee is often spared from the pain. Sensitivity disorders in the form of tingling and pins and needles can also occur. Since the spinal nerve is not affected in pseudoradicular pain syndromes, the sensitivity disorders cannot be assigned to any dermatomes (the area of skin supplied by a spinal cord nerve).
In the case of radicular pain, as occurs in a herniated disc, there is irritation of the nerve root. Accordingly, the pain and sensory disturbances radiating to the extremity are dermatome related.
The second leading symptom besides back pain is groin pain.
From a functional point of view, if groin pain occurs, the doctor should examine the following areas of the body:
- The ISG
- The hip joint
- The lumbar spine
- The thoracolumbar transition (exercise of the thoracic to the lumbar spine)
The SIJ can cause pain for a number of reasons.
Read more on the topic: ISG pain
From symptom to diagnosis
Prerequisite for diagnosing a ISG blocking First of all, a good anamnesis, which gives you important information about the correct region of the body and the dysfunction.
After the inspection, changes in the husbandry pattern are recognized and documented physical examination.
There are a number of tests that the doctor can use to identify a blockage.
It should be expressly pointed out that not all ISJ tests are described here, but rather examples are shown of how to get from symptom to diagnosis of ISJ blockage relatively quickly.
- Orientation tests
- Hip-drop test (Checking the pelvic depression)
The doctor stands behind the patient and asks the patient to alternately lower the free leg side, paying attention to the symmetry of the movements with regard to the lowering of the pelvis and the pelvic rotation.
Evaluation:
If the hip-drop test is physiological (lowering of the pelvis on the same side), the suspicion that the disorder is not in the functional chain of the lumbar spine-hip-SI joint and the examination can be started on the next higher floor. This is the thoracolumbar transition (TLÜ).
Is the hip-drop test reduced, there may be a fault in the ISG in which Lumbar spine, or in hip joint. A shortened iliotibial band or piriformis muscle can also lead to a decreased hip-drop test. If the test is reduced, further tests are available to the doctor or therapist in order to diagnose a disorder in the functional chain of the lumbar spine-ISG-hip.
With regard to the ISG, the next recommended diagnostic step is the
- Patrick Kubis test
The patient lies on his back and places his heel next to his opposite one Knee joint and performs a test movement in which the bent leg is guided in abduction (spreading apart) and external rotation. The aim of this test is to check the range of motion and the end feel of the ISG to test. The prerequisite for this test is that the hip joints, internal rotators, extensors and adductors are undisturbed.
Through these tests, the doctor has initial indications for a Malfunction of the SIJ, there are a number of ways to diagnose a blockage in the SIJ.
2. Joint play tests
- Preroll test
In this test, the joint play of both Sacroiliac joints tested in motion.
The doctor stands behind the patient and feels the posterior superior iliac spine from below (SIPS / posterior iliac spine). Then he asks the patient to curl up from the head and perform a maximum flexion of the trunk.
The lead behavior and the end position of the SIPS are observed. The movement of the Sacrum opposite the Ilium in the Sacrum joint tested. If the findings are normal, the two iliac spines are at the same height when the trunk is maximally flexed, exactly as in the starting position. This means free mobility in both sacroiliac joints. On the other hand, a one-sided elevation of the iliac spine at the end of the maximum trunk flexion speaks for a blockage of the corresponding ISG.
Usually the positive side is treated.
Practical tip
Since the forerun may also be purely muscular, it is advisable to hold the maximum flexion of the trunk for 20 seconds if the result is positive, as the forerun is through with a muscular cause Muscle relaxation can compensate.
ISG suspension test cum femore
The patient lies on his back and the examiner feels the sacroiliac joint space with his palpation finger. Then the examiner adjusts the patient's hip flexion so that the ISG movement can be felt on the palpation finger.
With a push along the longitudinal axis of the thigh, the final feeling of the SIJ can be felt and assessed. This test should always be carried out side by side.
There is a blockage on the side on which the joint play is restricted.
Lifting and shaking test
This test is done in the prone position. The examiner stands in a step position and grasps the anterior superior iliac spine (anterior iliac spine) with one hand while palpating the SI joint mobility with the other hand.
Then the examiner shakes the patient's ilium with one hand and feels the mobility of the ISG (shake test).
Another possibility is to slowly pull the ilium backwards, i.e. towards the examiner. You can feel the range of motion and the final feeling of the ISG (lifting test).
This test should also be carried out in a side-by-side comparison.
In all tests, the blocked side is the side of reduced joint play and is treated.
Differential diagnosis / alternative diseases

From a functional point of view, one differentiates between one Pelvic distortion and one ISG blocking.
The Pelvic distortion is actually a normal process when walking. But if there are functional disorders that are not caused by the ISG, but e.g. in the Spinepelvic distortion can also occur as a compensation mechanism in the head joints.
The Pelvic distortion is characterized by:
- an asymmetry of the pelvic position, the position of the pubic branches, or an indifference of the iliac spines on one side.
The ISG blocking usually does not have these asymmetries. - a positive forward phenomenon on the corresponding side, which disappears after 20-30 seconds with the trunk flexed to the maximum.
In the event of a blockage, the advance remains constant - normal joint play (joint play)
To the Pelvic distortion to treat, the cause must be found and treated.
It must be differentiated whether the cause is in the joint or in the muscles.
The Pelvic distortion and ISG blocking can also exist in combination.
therapy
There are a variety of Mobilization and manipulation grips around a ISG blocking to treat.
It must always be examined whether the cause of the complaints lies in the joint or in other areas as part of a pelvic twist, e.g. in the Musculature.
Also infiltration of the sacrum joint with a local anesthetic in combination with Cortisone can help improve symptoms.
In order to bring down the pain level, one should be supportive for a few days NSAIDs how Ibuprofen or Diclofenac in combination with a muscle relaxant (e.g. Sirdalud®).
After the treatment, the patient is recommended to move around and to take local warming measures (warm baths, hot water bottles, cherry stone pillows).
In general, one must add that disorders in the area of the sacroiliac joints are mostly secondary. For this reason, causes must be in the area of Spine and also the Hips be excluded.
If the symptoms do not improve after 2-3 treatments, inflammatory, rheumatological and tumor diseases must also be excluded.