Throat cancer
introduction
Of the Throat cancer (Syn. Laryngeal carcinoma, larynx tumor, laryngeal tumor) is a malicious (malignant) Cancer of the larynx.
This Tumor disease is often recognized late and difficult to treat. It is one of the most common malignant tumors of the head and Neck area.

Epidemiology
Of a Throat cancer mainly affects men between the ages of 50 and 70. They get sick about 10 times more often than women. In the Federal Republic of Germany about 3500 men and 500 women fall ill with a larynx tumor every year.
With regard to the mortality (mortality) of all cancers, the larynx tumor is overall a rare one Cancer. Approx. 1.5% of the male cancer deaths and about 1% of the female had cancer of the larynx.
Causes of throat cancer
In most cases, cancer of the larynx develops due to previous damage to the Larynx (Precancerous disease). Dysplasias are considered to be precancerous Leukoplakia and the carcinoma in situ.The most common causes of the development of a precancerous disease and the resulting larynx tumor are tobacco smoking and alcohol abuse. Viruses or environmental toxins such as asbestos can also promote the development of a tumor. A genetic predisposition can also promote the development of the disease.
to form
At all Larynx tumors it is squamous cell carcinoma. Larynx cancer is divided into different groups according to its location. These are located in the area of the glottis, which describes the entire vocal apparatus.
The glottis consists of Vocal cords and one Glottis. The Vocal cord cancer (Glottic cancer) is in the range of Vocal folds and the posterior wall of the larynx. The supraglottic carcinoma of the larynx lies above the vocal cords.
It is located in the area of the Epiglottis (epiglottis) and near the vocal cord pockets (Morgagni ventricle). From here some cancer cells can enter the surrounding area Lymph nodes scatter and form so-called metastases there. This is rare below the vocal folds Subglottic laryngeal cancer.
Hypopharyngeal carcinoma is a tumor that spreads in the lower part of the throat (Hypopharynx) trains. It is again differentiated into 3 affected regions: 90% of the hypopharyngeal carcinomas are in the Piriform Sinus, about 5% to the Back of the pharynx and another 5% in the Post-cricoid region.
A cancer of the larynx that spreads over the entire larynx is called transglottic laryngeal cancer designated.
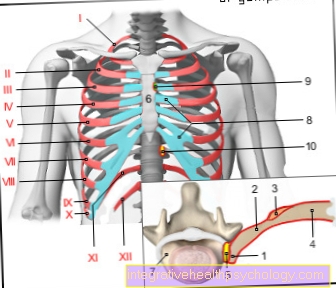
Figure larynx

- Epiglottis cartilage -
Cartilago epiglottica - Hyoid bone - Os hyoideum
- Thyroid cartilage-hyoid bone ligament -
Thyrohyoid ligament - Upper thyroid cartilage incision
Incisura thyroidea superior - Thyroid cartilage -
Cartilago thyroidea - Ring Cartilage Brace -
Arcus cartilaginis
cricoideae - Thyroid -
Glandula thyroidea - Ring band -
Ligament annular - Tracheal cartilage -
Cartilago trachealis - Nasal cavity - Cavitas nasi
- Oral cavity - Cavitas oris
- Throat - Pharynx
- Lungs - Pulmo
Airway L - L (blue)
Feed route S - S (red)
You can find an overview of all Dr-Gumpert images at: medical illustrations
Symptoms
Depending on their location, the individual forms of cancer differ in their symptoms.
The vocal cord cancer (Glottic cancer) is in the area of the vocal cords and quickly causes hoarseness. Since this leading symptom of larynx cancer often occurs early, the prognosis for vocal cord cancer is relatively good.
In some cases, cancer of the larynx can cause shortness of breath if the tumor has grown too large.
That too Supraglottic laryngeal cancer leads to hoarseness in a rough voice and possibly a feeling of pressure in the throat. Symptoms appear late, however, and this type of tumor metastasizes early to adjacent lymph nodes.
Because of this, the forecast of the supraglottic laryngeal carcinoma significantly worse.
Overall, subglottic laryngeal carcinoma is a very rare form and, due to its location below the vocal folds, does not lead to any specific symptoms.
In the later stages of throat cancer, you may experience shortness of breath, pain, and a feeling of pressure in the throat. The transglottic carcinoma and the Hypopharyngeal carcinoma also lead to hoarseness, shortness of breath or a feeling of pressure. This depends on the exact location.
You might also be interested in: What symptoms indicate throat cancer?
Diagnosis of throat cancer
The diagnosis of larynx cancer is often only made when the symptoms appear.
Then both are Smoking and Alcohol history, as well as the description of the symptoms pointing the way for further diagnosis.
By imaging like a Computed Tomography can he Throat cancer discovered and its position determined. In addition, affected lymph nodes can be detected by their size in the CT.
In order to get an exact picture of the spread of the tumor, however, is the Larynxoscopy (Laryngoscopy) essential. A small camera is pushed towards the larynx and it is examined closely. Since the examination is uncomfortable and the gagging stimulus that cannot be suppressed occurs in many patients, the throat area is numbed with an anesthetic spray.
To determine the exact type of tumor, a small sample is taken from the tumor (biopsy) and examined them histologically.
Therapy options for throat cancer
In most cases, only surgery with removal of the larynx is possible.
The larynx can be removed completely or only partially.
In the early stages of the tumor, organ-preserving removal can be done with a laser. In later stages, the larynx must be completely removed. The removal of the entire larynx (Laryngectomy) has significant consequences for affected patients. This primarily includes the loss of the voice. The so-called esophageal replacement language can be learned through a lot of training with a speech therapist.
Furthermore, there are electronic speech aids that enable a language. In both cases, however, the voice is no longer comparable to the original voice and it takes a lot of training to learn to speak again.
Furthermore, the trachea and the esophagus must be completely separated in order to avoid constant aspiration (Ingestion of food or saliva) to avoid.
This leads to a dehydration of the nasal mucosa with a loss of the sense of smell.
Every operation is followed by radiation (radiation therapy) and / or chemotherapy. If the tumor is still small, an attempt can be made to treat it without surgery but only with chemotherapy and radiation therapy.
If the tumor has spread to adjacent organs or lymph nodes, these must also be removed as part of a neck dissection.
Tumor stages and forms
Glottic carcinoma: The vocal cord tumor is divided into different stages. These are based on the spread of the tumor and determine the treatment options.
Stage T1 describes a tumor that is limited to the vocal folds. If necessary, the anterior and posterior commissures are also affected, the mobility of the vocal folds is preserved. If the tumor only affects one vocal fold, this is described by stage T1a; if both vocal folds are affected, it is referred to as stage T1b. In stage T2, the tumor has spread to the area above and / or below the vocal folds (supraglottis and / or subglottis). The mobility of the vocal folds is restricted.
Read more about the topic here: Vocal cord cancer - you should know about it
In stage T3, the tumor is limited to the larynx and the vocal folds are no longer mobile.
Stage T4 describes a spread to the thyroid cartilage and other organs outside the larynx.
The therapy of the vocal cord tumor is based on the above-mentioned classification. Nowadays, in the T1 stage, the tumor can usually be removed by laser surgery. The vocal cords and thus the language can be preserved. As a rule, this therapy is followed by radiation to kill all tumor cells.
Removal of the entire larynx (Laryngectomy) is mainly used in advanced tumor stages with restricted mobility of the vocal folds. In stage T2 and partially T3 it is possible to remove only the affected part of the larynx (Partial resection).
If the tumor has spread to the regional lymph nodes, numerous lymph nodes and other cervical organs must be consistently removed (Neck dissection). If the tumor was discovered at an early stage, the 5-year survival rate is 90%.
Supraglottic carcinoma: This type of larynx tumor spreads in the area of the epiglottis and pocket folds.
If the tumor is at an advanced stage, it can often be seen that it has spread to the vocal cords, the opposite side or a breakthrough into the underlying fatty tissue. A computed tomogram (CT) or magnetic resonance imaging (MRI) scan can be performed to assess tumor infiltration.
The ultrasound (Sonography) used. Laser surgical removal of the tumor is also possible with this type of tumor in stages T1 and T2. If the tumor is localized on one side only, partial removal of the larynx (Hemilaryngectomy) respectively. However, supraglottic carcinoma is often well advanced by the time the diagnosis is made. In this case, the entire larynx must be removed. In the event of metastasis or spread to neighboring organs, neck dissection must be carried out.
With this larynx tumor, the 5-year survival rate is only around 60%.
Subglottic carcinoma: a laryngoscopy is performed to establish the diagnosis (Laryngoscopy) and an ultrasound scan (Sonography) of the neck. Magnetic resonance imaging (MRI) or computed tomography (CT) is then performed to assess the extent of the tumor.
Panendoscopy is a special feature of this tumor. An endoscopy of the throat, nose, esophagus, larynx and windpipe is performed. During the examination, samples are taken at various points in order to be able to classify the tumor precisely. As a rule, the entire larynx must be removed for this tumor (Laryngectomy).
If it spreads beyond the larynx, neck dissection is also carried out. The 5-year survival for this tumor is 50%.
Hypopharyngeal carcinoma: Hypopharyngeal carcinoma grows in the lower part of the throat and is also diagnosed by a larynxoscopy. In the earlier stages, the tumor is located on the back wall of the throat.
In advanced stages, the tumor has spread to the larynx, thyroid, and muscle fascia above the vertebrae. Various biopsies are taken during the examination.
Ultrasound, computer tomography and magnetic resonance imaging of the neck, abdomen and chest are used to assess the extent of the tumor. In the T1 and T2 stages, an organ-preserving partial resection of the throat can be carried out if no lymph nodes are involved. In the case of extensive tumor growth, a part of the hypopharynx is removed in combination with a larynx removal, neck dissection and subsequent radiation. As an alternative to surgery, chemotherapy with a platinum-containing chemotherapeutic agent (cisplatin, carboplatin), as well as 5-fluorouracil, bleomycin, mitomycin and methotrexate can be performed. Often this is also done in combination with radiation.
In the end-stage of the tumor, gastrostomy and tracheotomy are often necessary for ventilation and nutrition.
The 5-year survival is very low with this tumor. In the case of a T1 or T2 stage, the probability of survival is around 30%, in advanced tumor stages only around 20%.
forecast
The prognosis depends on the location and stage of the larynx cancer. So has it Glottic cancer in the area of the vocal folds a significantly better prognosis than that supraglottic carcinoma, which lies above the vocal folds and quickly metastasizes.
The prognosis in this case depends on the extent of the tumor growth when the first symptoms appear. The Saarland Cancer Register describes a 5-year survival rate of 65.4% for men and 75.8% for women. However, these numbers are very general and are not seen as a function of tumor stage and location.
Summary
Larynx cancer is a relatively rare but dangerous tumor of the larynx and adjacent organs.
The main cause of the formation of such a tumor are pollutants such as nicotine and alcohol. Larynx cancer can be localized in different parts of the larynx and is divided accordingly into different groups.
The therapy options and chances of recovery depend mainly on the localization. A distinction is made between glottic carcinoma, supraglottic and subglottic carcinoma, and hypopharyngeal carcinoma. Depending on their localization, the individual tumor types can trigger symptoms sooner or later. This explains the difference between the various chances of recovery.
The therapy options are primarily surgical in the context of a complete or partial removal of the larynx.
In the very early stages, laser surgery and organ preservation can also be performed.
In later stages, the removal of neighboring organs and lymph node packages is necessary in order to achieve freedom from tumors. Most operations are complemented by radiation and / or chemotherapy.
Cancer of the palate is one of the carcinomas of the oral cavity. In the following article, you will find out how to recognize palatal cancer and how it is treated if you are present: Palate Cancer - Things to Watch Out For











.jpg)