Meniscus lesion
Synonyms
Meniscus tear, meniscus tear, meniscus rupture, meniscus damage
English: meniscus tear
definition
The term Meniscus lesion (also: meniscus tear, meniscus rupture, meniscus injury) denotes damage to the Internal or external meniscus of the knee. Of the Medial meniscus is affected by lesions far more often than the External meniscus, because it is attached to both the joint capsule and the inner ligament and is therefore less mobile. Most common such a lesion is through direct Violence for example at Sports or by, mostly age-related, Signs of wear (degeneration) conditional.
Anatomy of the menisci

Excursus meniscus:
The meniscus consists of two crescent-shaped fiber cartilage discs, which are positioned between the thigh and lower leg in order, as mentioned above, to prevent the incongruence (inequality) to equalize the articulating bones and thus to transfer shocks evenly to the cartilage of the lower leg. In addition, the meniscus distributes the synovial fluid, which is particularly responsible for protecting the cartilage tissue, as it causes cartilage discs to slide over one another without friction. It also supplies the cartilage tissue with nutrients and is responsible for removing waste materials from the joint space.
The diagram on the right shows the anatomical structure of both menisci.
In the middle, the two menisci are separated by the cruciate ligaments, to the left of the cruciate ligament is the outer meniscus (light blue color), to the right of the cruciate ligaments is the medial meniscus (greyish color). and the posterior cruciate ligament. As you can easily see from the diagram, the volume of the outer meniscus is significantly larger than the volume of the inner meniscus.
Appointment with a knee specialist?

I would be happy to advise you!
Who am I?
My name is I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
The knee joint is one of the joints with the greatest stress.
Therefore, the treatment of the knee joint (e.g. meniscus tear, cartilage damage, cruciate ligament damage, runner's knee, etc.) requires a lot of experience.
I treat a wide variety of knee diseases in a conservative way.
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- - your orthopedic surgeon
14
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
Further information about myself can be found at
Illustration of the menisci

- Inner meniscus -
Meniscus medialis - Inner articular knot
(Shinb.) -
Medial condyle - Transverse ligament of the knee joint -
Lig. Transversum genus - Kneecap ligament -
Ligamentum patellae - Bursa - Bursa
- Outer meniscus -
Lateral meniscus - Outer joint nodules
(Shinb.) -
Lateral condyle - Anterior cruciate ligament -
Lig. Cruciatum anterius - Posterior cruciate ligament -
Ligamentum cruciatum posterius - Femur - Femur
- Shin - Tibia
- Kneecap - patella
You can find an overview of all Dr-Gumpert images at: medical illustrations
to form
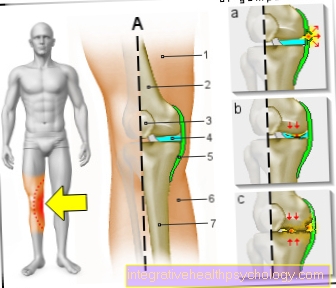
There are different degrees of severity and different shapes of meniscal lesions. If the meniscus is merely squeezed, it is called a contusion (see: Meniscus squeezing).
However, if it is actually torn, a distinction is made between three types of tear: In the case of a radial or flap tear, the line extends from the inner edge of the meniscus outwards; in the case of a horizontal tear, the tear runs horizontally, and in the case of a basket-handle tear, the tear runs longitudinally through the meniscus.
A basket handle tear harbors the risk that a free edge slips into the joint space and thus leads to worse complaints. The rear horn is particularly often affected in a tear, among other things because it has the poorest blood supply.
Grade 1 - 4 of the meniscal lesion
A Meniscus lesion, so a tear, tear or degenerative change in a meniscus can be caused by a injury (Trauma), through to the other Signs of wear be conditional. Depending on the severity of the lesion, they are divided Meniscus lesion in 4 degrees of severity.
Grade 1-3 are due to wear and tear Grade 4 one speaks of one Meniscal tear.
- Is there a Grade 1 meniscal lesion before, so is the damage to the meniscus centrally located, small and punctiform. As a rule, the patient notices nothing or very little of this.
- A 2nd degree meniscal lesion runs horizontally in the meniscusbut does not reach its edges.
- Of the 3rd degree meniscus damage differs from the 2nd degree mainly by the length, or the Size of the lesion.
- At the 4 degrees the injury is enough to the edge of the meniscusso that a deep crack appears. These cracks can be found in different subclasses subdivide. The most common are the Radial crack and the Basket handle tear. Of the Radial tear “divides” the meniscus in half, at a Basket handle tear tear the inner parts, so that a "handle-shaped" space closed off from the outside is created. Such patterns of injury are by means of imaging, diagnostic procedures like magnetic resonance imaging (MRI for a meniscus tear) clearly visible. Patients with a Meniscus lesion grade 4 usually show clear symptoms, such as Pain and restricted mobility.
Causes of a meniscus lesion
In principle, anyone can suffer a meniscus lesion, but athletes on the one hand and elderly people on the other hand are predisposed to this. There are about twice as many men as women among the patients. The movement that causes most meniscal lesions is a combination of a rotational movement combined with a pressure load. Such movement can occur in certain sports, such as soccer or skiing. Younger people in particular are affected by this form of meniscus injury.
In older people, however, there is often no direct trigger of a meniscus tear at all. This is due to the fact that the cartilage tissue of the menisci is heavily and sometimes overstrained over time, whereby more and more smaller cracks form. These remain unnoticed for a long time, until at some point a slight load leads to the meniscus finally tearing. This form of meniscus damage mainly affects people over the age of 40.
Symptoms of the meniscus lesion

The complaints a patient has with one Meniscal tear describes differ depending on the severity and location of the meniscus lesion. Frequently when a trauma caused the crack, first of all a Cracking or Snap noticed above the joint space. In addition, the person affected suddenly feels Pain (depending on the torn meniscus either outside or inside of the knee) Bow or stretch, especially with Go, amplify.
The meniscus itself is not responsible for the pain, since the cartilage tissue is not supplied with nerves, but torn fragments can Joint capsule irritate. Sometimes this creates a Joint effusion, an accumulation of fluid in the knee joint that can be seen as swelling. In some cases, part of the meniscus slips into the joint space and thus “blocks” the knee joint. The result is that neither extension nor flexion is possible in the joint. Sometimes an injury to the medial meniscus is associated with one Rupture of the anterior cruciate ligament and des inner collateral ligamentwhat you then call "Unhappy Triad" designated. With this injury there is usually an additional one Hemorrhage into the joint and the signs of cruciate and collateral ligament damage are positive.
Diagnosis and therapy
The diagnosis of a meniscus lesion requires a medical history and a subsequent clinical examination. Various Meniscus mark getting tested.
These include, among other things Steinmann I sign (Pain arises from Medial meniscus lesion for external and external meniscus lesions with internal rotation), the Steinmann II sign (with bent Knee joint the pain moves dorsally), that Payr sign (When sitting cross-legged, the pressure on the inner joint space causes pain in the presence of an internal meniscus tear) Apley test (the patient lying on his stomach feels pain when the knees are bent to a 90 ° angle and pressure is exerted on the soles of the feet in this position during internal or external rotation) and the release of Varus and valgus stress, causing pain through compression, should there be an injury to the meniscus.
It can also be useful in some cases to use a X-ray image to discover any bony injuries. You also run a Jointoscopy (Arthroscopy of the knee) by (eliminating the use of the Magnetic resonance imaging for a meniscus tear (MRT) is now usually no longer needed), in which the treatment can usually be included.
In the Arthroscopy of the knee either parts of the meniscus can be removed (Meniscectomy), whereby one should take care to remove as little tissue as possible to avoid a later arthrosis of the knee joint or suturing the meniscus, a technique that should be done especially in younger patients.
The long-term prognosis of those affected depends on the extent of the damage and the corresponding therapy. It is advisable to seek advice from a doctor or physiotherapist in order to ensure that the knee is adequately and not too quickly stressed again. Often after about three months the ability to actively participate in sport is restored, but some patients never regain their previous knee resistance after a meniscus tear.
MRI for a meniscus tear
Using MRI, over 95% of meniscus tears can be diagnosed and MRI is the gold standard for detecting a meniscus tear without performing an invasive procedure. In MRI, the contrast in the tissue creates a three-dimensional formation without radiation exposure generated.
Unfortunately, some meniscus tears cannot be seen on the MRI or the tears are worse on the arthroscopy than would be suspected on the MRI. Due to the constant improvement in MRI technology, the error rate in MRI in meniscus tears has decreased significantly.
Figure meniscus tear

Meniscal tear
(= Meniscus rupture)
I - longitudinal tear
II - oblique view (rag tear)
III - radial crack (transverse crack)
IV - basket handle tear (special form)
V - degeneration (wear and tear)
- Inner meniscus -
Meniscus medialis - Outer meniscus -
Lateral meniscus - Posterior cruciate ligament -
Lig. Cruciatum posterius - Anterior cruciate ligament -
Lig. Cruciatum anterius - Femur -
Femur - Kneecap - patella
- Shin - Tibia
You can find an overview of all Dr-Gumpert images at: medical illustrations
Operation meniscal lesion
To the Stability in the knee joint To restore and avoid consequential damage such as osteoarthritis after a meniscus lesion, surgery can be considered. Nowadays, knee operations are usually minimally invasive Knee reflection (Arthroscopy) performed. The required instruments and a mini camera are inserted into the joint through the smallest incisions in the skin. There are three different approaches to such an operation.
- Partial meniscal resection: A partial meniscus resection is the partial removal of the affected meniscus. This removes the parts that are torn and therefore no longer functional. It is crucial in this procedure that not too much and not too little tissue is removed. The lesion must be removed, but the stability of the joint must not be compromised.
- Meniscus suture: If the broken meniscus is not damaged too much, the surgeon can try that to sew up torn fabricsso that the two parts grow back together.
- Meniscus replacement: If the meniscus is badly damaged, it may be necessary complete removal to carry out the same. Then it has to Cartilage discs but replaced otherwise it quickly becomes wear-related Knee osteoarthritis comes. Complete removal of menisci is therefore extremely important rarely used procedure.
advantages a meniscus operation are very much thanks to a minimally invasive procedure short hospital stays from 1-3 days and the shortened total therapy time. Despite these advantages, the meniscus operation is a procedure that is performed under general anesthesia and therefore involves the usual risks of an operation. Whether or not an operation can be performed on a meniscus lesion therefore depends on the patient Age and physical condition of the patient from.
Treatment without surgery
If the patient's physical condition does not permit or is it an operation slight meniscus lesion, can a conservative therapy, i.e. therapy without surgery should be considered. Here you should know that destroyed Cartilage tissue rarely heals on its own. In conservative therapy, the cause is not actually treated, but rather just the symptoms.
Conservative therapy always starts with Combating pain with pain relievers (Analgesics). Medicines with active ingredients such as ibuprofen or acetylsalicylic acid are suitable for this. If an operation has not yet been ruled out, caution should be exercised when taking some medication, as it can have a blood-thinning effect (e.g. when taking aspirin). Medication should therefore be taken for meniscus lesions, especially over a long period of time always clarified with a doctor become.
To Forearm crutches can provide relief to be used. Also Bandages or splints on the knee can help relieve pain. If the symptoms have improved, each patient can do their own part to ensure that the symptoms of the meniscus lesion do not worsen again.Various preventive measures make everyday life easier. For example should Sitting for long periods of time as well as “squatting” should be avoided and the knee should also be protected during sport and exercise Value. There are especially for athletes special, stabilizing sports bandagesthat can be worn with increased stress. Physiotherapy or physiotherapy can help after symptoms subside Stability in the knee joint to improve again.