Finger osteoarthritis surgery
Operative measures for finger osteoarthritis
If conservative forms of therapy have not led to the desired success, the attending physician can consider surgical therapy. Usually a operational measure only considered if the symptoms have persisted for a long time and the joints are already severely deformed. These deformations can lead to joints deviating completely from the finger axis.

As part of the finger osteoarthritis operation, not only the heberden nodules are usually removed. In addition, the swollen joint mucosa is usually removed. Another option is to cut the pain nerves that supply the end joint. It should be noted that the sensory nerves are not affected by a transection and therefore only rarely do sensory disorders occur in the area of the fingers or fingertips.
In patients who, in addition to severe pain, already have severe deformations of the joints, the affected joint is usually stiffened as part of the finger arthrosis operation during the procedure. Mobility usually remains in the other joints, so that the affected finger does not become completely rigid, i.e. it is still fully mobile in some areas. The affected joint is stiffened either by inserting two to three small wires (so-called Kirschner wires) or by inserting special screws.
In the area of surgical therapy, too, advantages and disadvantages must be weighed against one another. The advantage of this surgical method is, for example, that the mobility of the end joint can be preserved.
However, it must be pointed out that in the long-term course of the disease, patients may be affected by the disease again and thus similar problems may recur. It is also possible that pain may persist for a long time after the operation. Surgical intervention is therefore no guarantee of eliminating the disease in the affected joint.
What happens to the inserted wires?
The wires inserted during the operation can only be removed when it has been ensured by radiography that the arthrodesis (joint stiffening) has been completely built through. As part of a minor surgery, the wires are usually after 6 to 18 months away. When this happens in each individual case must be decided individually.
An alternative to the surgical removal of the wires is the possibility of leading the wires out of the skin after the operation. Then they can be done without further surgery and usually after about 6 weeks removed. The risk that the desired stiffening of the joint will not take place and that the surgical procedure will fail is very high.

I would be happy to advise you!
Who am I?
My name is I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
In order to be able to treat successfully in orthopedics, a thorough examination, diagnosis and a medical history are required.
In our very economic world in particular, there is too little time to thoroughly grasp the complex diseases of orthopedics and thus initiate targeted treatment.
I don't want to join the ranks of "quick knife pullers".
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me at:
- - orthopedics
14
Directly to the online appointment arrangement
Unfortunately, appointments can only be made with private health insurers. I ask for understanding!
Further information about myself can be found at -
Risks
In principle, no operation without risk applies to any form of surgical therapy! At this point, however, possible risks can only be pointed out by way of example. In addition, only the attending physician can discuss individual risks with you and take them into account as part of the therapy. A possible risk for the failure of the finger osteoarthritis operation is that the arthrodesis does not build through and thus the desired joint stiffening does not occur. Premature loosening of the wires is also conceivable.
Every surgical intervention carries the risk of developing Infections. While in the case of superficial infections it is usually sufficient if a local antiseptic treatment is carried out in combination with an antibiotic, a revision operation (second intervention) may be necessary for the rarely occurring deep joint infections.
In addition to the risks already mentioned, there is a rare risk of developing a so-called Sudeck dystrophy. This refers to the painful swelling of the hand, which can severely limit the mobility of the hand as a result of the impairment of the fine blood circulation. The cause of the development of this clinical picture is largely unknown.
anesthesia

What kind of anesthesia is used during this procedure?
The so-called Plexus anesthesia, when operations are performed on the hand. An anesthetic is injected into a plexus of nerves in the armpit, which numbs the entire arm after about 30 to 45 minutes.
In addition to minor surgical interventions, plexus anesthesia is also suitable for major operations. A positive aspect to be emphasized here is the significantly lower risk of anesthesia and the fact that the patient is almost fully functional again immediately after the operation. While the arm is still numb for hours and thus the pain can almost be eliminated, it can be addressed and can, for example, eat and drink.
Since the patient would be fully aware of the operation with this form of anesthesia, it is possible to inject a light sleeping pill. The patient then sleeps through the operation, but not with the anesthetic sleep general anesthetic may be confused.
Aftercare
What happens to the finger after the operation? The operated finger is bandaged in the first few days after the operation. In addition, both the operated finger in the area of the middle and end joint and the entire wrist are immobilized in order to reduce pain. A few days after the operation, the immobilization usually only applies to the operated joint.
If the healing goes as planned, the amount is Immobilization for about six weeks. However, this may vary from person to person and is usually prolonged with the occurrence of complications.
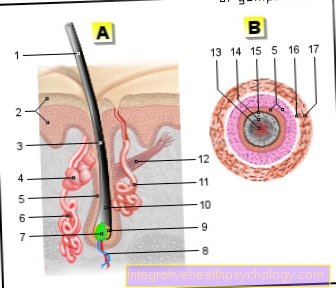
Illustration of a finger osteoarthritis

I - finger joint line - green
II - mid-finger joint line - blue
III - saddle thumb joint line - purple
- Distal phalanx - Phalanx distalis
- Phalanx - Phalanx media
- Phalanx - Ph. Proximalis
- Metacarpal bones - Metacarpals
- Trapezoidal leg - Trapezium
- Trapezoid leg - Trapezoid bone
- Scaphoid bone of the hand -
Scaphoid bone - Articular surface with articular cartilage -
Articular facies - Joint capsule - Articular capsule
a - Healthy joint
b - arthritis (inflammation of the joints)
c - osteoarthritis
A - Back of the right hand
B - osteoarthritis of the finger joint
= Heberden osteoarthritis (green line)
Mid-finger joint arthrosis
= Bouchard osteoarthritis (blue line)
C - Thumb saddle joint arthrosis
= Rhizarthrosis (purple line)
You can find an overview of all Dr-Gumpert images at: medical illustrations

.jpg)