Pneumothorax
Definition of pneumothorax
Under a Lung collapse / pneumothorax (pneu = air, thorax = chest) one understands the penetration of air into the lung space (pleural space), which leads to the collapse of the lung tissue.
The causes for this can be a broken rib, but the bursting of distended lung tissue (pulmonary emphysema).

Classification / forms
The lung membrane (pleura) consists of two sheets or layers.
The pleural space or gap lies between the two leaves of the pleura. The negative pressure that normally prevails in the pleural space is released in a pneumothorax and the lungs contract due to their inherent elasticity.
You can think of it as giving water between two plates. The glass plates can now move easily against one another, but cannot be separated from one another.
If, apart from the pneumothorax (lung collapse), there is no underlying lung disease that can be identified radiologically (on the X-ray), it is called a primary pneumothorax.
However, if the x-ray shows a previous lung disease, it is a secondary pneumothorax.
Read about this too Pleural puncture
The tension pneumothorax is a special form. With tension pneumothorax, air penetrates the pleural space from the outside (e.g. through a knife, broken rib). With every inhalation, more air accumulates, which displaces and compresses the soft and elastic lung tissue. The valve mechanism prevents the air from escaping when you exhale. The heart is pushed to the opposite side.
The division can also be made into internal and external pneumothorax.
An internal pneumothorax arises within the lungs (e.g. due to the bursting of alveoli in pulmonary emphysema), whereas an external pneumothorax e.g. caused by a knife stab or a broken rib that pierces the lungs. The pneumothorax is often accompanied by a serous (seropneumothorax), purulent (pyopneumothorax) or bloody (hemopneumothorax) effusion.
Bilateral (bilateral) pneumothorax is present in almost 1-2% of cases.
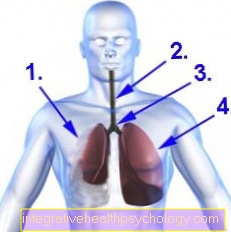
Pneumothorax
- collapsed lung
- Windpipe (trachea)
- Tracheal bifurcation (Carina)
- left lung with full development
causes
The cause of a primary pneumothorax usually lies in the rupture (tear) of alveoli (occurs particularly in the case of emphysema).
Inflammation of the lungs (pneumonia) and lung cancer (bronchial carcinoma) can cause a secondary pneumothorax, among other things. This clinical picture can also be caused by improper pleural puncture (e.g. as part of CSF diagnostics) or acupuncture treatments in the lung area.
The inner pneumothorax / lung collapse is caused by the bursting of alveoli (e.g. due to a lack of protein). For example through a broken rib when the lung tissue is pierced.
You can find more information under our topic: Broken ribs
The tip of the lung can also be injured and a pneumothorax caused when the needle is inserted as part of a stellate ganglion blockade. Read more about this under: Stellate ganglion blockage
Symptoms / complaints
The symptoms include:
- shortness of breath
- Chest pain and
- rapid breathing (Tachypnea).
A tension pneumothorax results in compression (squeezing) of the lungs and displacement of the central part of the chest cavity in which the heart is located (mediastinum / mediastinal displacement) to the opposite healthy side. The lung compression causes shortness of breath (dyspnoea) here too. Another symptom of tension pneumothorax is shock. It should be noted at this point that this is an emergency.
Also read: Stitching in the right chest
diagnosis
The physical examination reveals a darker (so-called hypersonic) knocking sound over the affected area and a missing or even weakened breathing sound.
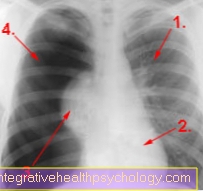
The pneumothorax can be a very impressive finding in the X-ray image.
The findings are best seen after exhaling (expiratory exposure). The collapsed lung is represented by a decrease in transparency (less blackness) compared to the healthy side.
The pleural space, which is now filled with air, is dark / black. A vessel drawing (white lines) is not visible. In the case of a tension pneumothorax, the mediastinal displacement can also be seen here:
The heart shadow is shifted. The CT (computer tomography) shows a similar picture: the affected side is darker (black) than the healthy one, on which the intact lung tissue can be seen as whitish markings. Air appears as a uniform black in both X-rays and CT (computed tomography).
X-ray with pneumothorax
In an acute situation, conventional X-rays are the fastest way to find out the cause of the patient's symptoms, such as shortness of breath or circulatory crises. Further diagnostics should only be considered if the cause of the pneumothorax is unclear. The X-ray image is taken while standing in two planes, i.e. from the front or back and from the side of the patient. Even after a chest drain has been placed, an X-ray is used to check the optimal position of the tube in the chest.
Read more on the topic: Chest x-ray (chest x-ray)
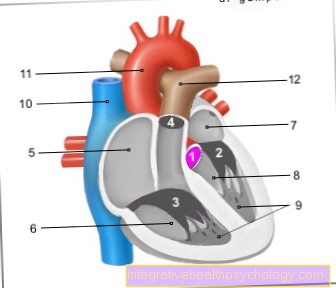
X-ray pneumothorax
- left lung (normal)
- heart
- collapsed right lung
- Air in between the lung membrane
CT for pneumothorax
Computed tomography (CT) can be quite helpful as a diagnostic tool in the event of ambiguities in conventional X-rays. For example, if there is a suspicion of an underlying disease that is responsible for the pneumothorax, computed tomography can be a pioneering tool to find out the cause.
With regard to the spontaneous pneumothorax already mentioned above, the CT can give a more precise prognosis as to whether such a case can repeat itself, because fine changes in the lungs can be better represented here than in the conventional X-ray image. Compared to conventional x-rays, the tomographs of the computed tomography allow a more precise localization of the cause.
Ultrasound for pneumothorax
The ultrasound examination of a patient with suspected pneumothorax is initially not very effective. Due to the technical properties of the ultrasound process, air in the ultrasound has a partially obstructive effect on the actual examination. It behaves differently if there is more fluid in the pleural space. This can be proven well. In general, if a pneumothorax is suspected, the two examinations already mentioned can be preferred. The normal X-ray simply offers the best representation of the problem in its overview.
therapy
A small pneumothorax can initially be observed and the spontaneous regression can be accelerated by administering nasal oxygen.
A symptomatic pneumothorax, that is, a pneumothorax that causes health problems for the affected person, can be treated with suction of air through a tube. This method is applied as a so-called thoracic drainage with suction.
If there is no complete regression or if the disease recurs, part of the lung tissue can be removed in exceptional cases (pleurectomy).
How is the chest tube placed?
The first step is to select the appropriate location on the patient's chest. There are essentially two places where a chest drain can be placed. One lies in the area of the middle lateral rib cage between the 4th and 5th rib. The drainage introduced here is then called the Bülau drainage.
The second option is called Monaldi drainage and is inserted into the upper middle chest between the 2nd and 3rd ribs.
Local anesthesia is applied before the drainage system is installed, which can divert secretion or blood and air. Then a small skin incision is made with a scalpel and the upper edge of the lower rib is worked with scissors or pliers. This takes place until the corresponding space, the so-called pleural space, has been reached. This lies roughly between the chest and the lungs. After the drain has been placed, it is attached to the patient with a skin suture and a plaster is applied. Then the connection to a closed system consisting of a water lock and a secretion container, which is put under suction. The correct fit and the therapeutic effect of the chest drain are then checked using an X-ray.
Read more about this under: Chest drain
How is the chest tube removed?
The decision to remove a chest drain is made by the attending physician after several days of observation. Test phases are repeatedly carried out in which the suction is switched off on the drainage. This is followed by an X-ray to see whether there is renewed accumulation of air or fluid in the pleural space. If this is not the case, the drain can be removed. This takes place under suction and tension on the hose. The existing hole in the skin is then covered with a sterile compress and initially also compressed with a bandage.
How long is the chest tube in place?
The drainage was created for a certain indication, a reason. If this reason has been eliminated or the triggering factors have been minimized, the removal of the drainage can be considered. Thus, it differs from case to case how long a chest tube has to remain in place. After careful consideration, the medical team in the hospital then makes a joint decision. Broken down, it can be said that the drainage is pulled when there is no further accumulation of air or fluid in the pleural space. Usually this is the case after a few days. A chest drain can also be left in place for several weeks.
When do you need surgery with a pneumothorax?
Surgical therapy should be considered in the event of recurrent symptoms associated with pneumothorax. Proven weak points in the lung tissue, called “bulla” (bladder) in technical terms, should also be surgically repaired. These are thin-skinned, protruding bubbles that can burst spontaneously. The scenario of a tension pneumothorax also requires surgical treatment. If chest tube therapy is inadequate and air leaks continue, surgery should also be considered. In the case of rib fractures, which are the cause of a pneumothorax due to splinters or fracture fragments, an operation should be performed to eliminate the problem.
During the operation in general, potential leak points are sewn over or smaller parts of the lung are resected. In addition, a so-called pleurodesis can be helpful to prevent the lungs from collapsing. The lungs and pleura are glued together. These two skins form the outer boundary of the pleural space, which lies between the inner chest and lungs.
How long does it take for a pneumothorax to heal?
The time it takes to heal a pneumothorax can vary, depending on the cause and extent of what is happening. With so-called spontaneous pneumothorax, for example, alveoli can burst without external causes and lead to air flowing into the pleural space. This can improve after a chest drain is placed. However, if it occurs frequently, surgical remediation of the cause may be necessary.
In another example, the tension pneumothorax, as with all forms of pneumothorax, air flows into the pleural space, but this air does not escape. The air collects in the pleural space without being able to be exhaled. In this case life-threatening circulatory arrest can occur if the organs in the chest, such as the heart, are relocated, i.e. pushed aside. The tension pneumothorax is always an absolute emergency, which is why the healing here is in many cases more protracted than with a spontaneous pneumothorax.
prophylaxis
There is no actual prophylaxis for the pneumothorax. One can only try to prevent the underlying diseases of the lungs.
forecast
In a spontaneous pneumothorax, e.g. In the case of emphysema treated with chest drainage, the recurrence rate (recurrence rate) is 20 - 50%
After drug or surgical therapy, the recurrence rate is 0-10%. The tension pneumothorax, which is an emergency, is life-threatening.
Can a pneumothorax be fatal?
In principle, inadequate or lacking treatment can result in death. This also explains the urgency with which one should proceed. The danger lies in insufficient ventilation of the affected lung. You only breathe with half your lungs, so to speak. This becomes noticeable to the person affected by pronounced shortness of breath combined with pain. It can also lead to circulatory instabilities and even shock, which endanger the life of those affected. If a so-called tension pneumothorax develops, there is not only severe shortness of breath, but also an increased lack of oxygen supply to the body, which can also trigger fear, restlessness and even panic. Since this is an acute, life-threatening clinical picture, if left untreated, the person affected will die.
What can be the consequences of a pneumothorax?
The first consequence of a pneumothorax is the recurrence. This is most likely with a spontaneous pneumothorax. Furthermore, delayed supply can lead to circulatory disorders up to and including cardiac arrest.
As a consequence of the supply of a thoracic drainage, infections can occur, which on the one hand can take place in the skin but on the other hand also in the lungs and / or pleura, as so-called pleurisy. The consequences of a pneumothorax caused by external injury can be unfavorable ruptures of ribs, but also the penetration of blood into the pleural space, which is known as a hemothorax. If the problem is corrected by an operation, a longer hospital stay can result. If part of the lung is resected during the operation, i.e. cut away for better care, the lung function can be impaired.
Pneumothorax during exercise
Pneumothorax can occur during exercise, especially in young and sporty people. On the one hand, traumatic, i.e. through external, pointed or blunt force that injures the chest. On the other hand, in addition to the traumatic form, there is also the more common spontaneous pneumothorax. This occurs more frequently in men between the ages of 15 and 35 who are slim and tall. Often these are smokers and have a genetic predisposition to develop pneumothorax. With increased exertion, this form leads to deeper, more strenuous breathing, which can then burst alveoli. Air now penetrates the pleural space and a pneumothorax has developed.
Pneumothorax after an operation
A pneumothorax can also develop after operations. If interventions are made on the chest to open up the pleural space, this is inevitable. For this reason, chest drains are always placed in this type of operation, which contribute to the healing process after the operation.
Certain other medical acts can also lead to a pneumothorax. When central venous catheters are placed, large veins near the neck or shoulders are punctured.Since the tips of the lungs are also in the vicinity, it is possible to unintentionally hit the lungs and thus produce a pneumothorax.
Symptoms of a pneumothorax in the baby
Basically, it can be said that the probability of pneumothorax in a healthy newborn is very low. It can be more likely in premature babies, as lung maturation is completed in the last few weeks of pregnancy. If this is not completed sufficiently, it can lead to respiratory distress syndrome. The symptoms that occur are shortness of breath, i.e. deepened and insufficient breathing that progresses at rest. In addition, the mucous membranes may initially turn blue, and then the skin as well. Other symptoms may include a drop in blood pressure or an inability to respond in the form of lethargy.
Read more about this under: Respiratory distress syndrome in the newborn