rickets
introduction
The rickets (Greek rachis, spine), is a disease of the growing Bone with impaired mineralization of the bones and disorganization of the growth plates in children.
She goes on a Disturbance of the calcium-phosphate metabolism back, usually through a too little intake or one Metabolic disorder is caused. In adulthood, rickets is called Osteomalacia designated.
frequency
The rickets is no reportable illness and is therefore difficult to pin down to numbers.
Statistically, however, it is striking that African-American children in particular are more frequently affected than others. The occurrence of typical symptoms, however, is very rare.
Most children only show one in a laboratory Vitamin D deficiency. This is found very often and also in highly developed countries. An American study showed that almost half of all girls had a significantly too low vitamin D level in their blood at the end of winter. Vitamin D deficiency also occurs epidemiologically in countries with high sun exposure, as women in these countries are often heavily veiled for religious reasons.
In European countries show especially infants and childrenwho are on a macrobiotic diet will show symptoms of rickets.
Calcium Phosphate Metabolism
The balance between Calcium and phosphate in the body is produced by the hormones calcitriol (vitamin D), and parathyroid hormone Calcitonin regulated.
The concentration of the two substances is closely linked and is precisely regulated.
The greatest amount of calcium and phosphate is in the form of the Hydroxyapatite in bone saved.
If the body registers too much or too little phosphate or calcium, parathyroid hormone is released. This releases calcium from the bones or builds it into the bones. Excess phosphate is over the Kidneys excreted or, in the case of a lack of phosphate, this is increasingly reabsorbed from the urine. The absorption of calcium is only possible with the help of vitamin D3, its production with the help of ultraviolet radiation from sunlight in the skin arises.
The vitamin D3 is then in liver and kidney via various precursors (25-hydroxy-cholecalciferol) ultimately converted into the actually effective calcitriol (1,25-dihydroxy-cholecalciferol) and enables calcium to be absorbed into the bones. If there is a lack of vitamin D3, the bones become increasingly fragile, since mineralization cannot take place and the typical symptoms of rickets occur.
Appointment with ?

I would be happy to advise you!
Who am I?
My name is I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
In order to be able to treat successfully in orthopedics, a thorough examination, diagnosis and a medical history are required.
In our very economic world in particular, there is too little time to thoroughly grasp the complex diseases of orthopedics and thus initiate targeted treatment.
I don't want to join the ranks of "quick knife pullers".
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You will find me:
- - orthopedic surgeons
14
You can make an appointment here.
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
For more information about myself, see - Orthopedists.
causes
There are basically two forms of rickets:
The more common form is Calcium deficiency rickets.
This is caused by a lack of vitamin D. This usually arises from a combination of one Insufficient vitamin D intake from food and at the same time too little sun exposure.
In rare cases there is a Enzyme defect responsible for the vitamin D deficiency. This is called Vitamin D-dependent rickets type 1 and type 2 designated.
Furthermore can other bowel diseases prevent sufficient vitamin D absorption from the intestine (Celiac disease, Cystic fibrosis).
Also certain drugs like Phenytoin and phenobarbital to Epilepsy therapy decrease absorption from the intestines and increase the breakdown of vitamin D3.
The rarer one Phosphate deficiency rickets leads to one increased loss of phosphate through the kidneys and thereby disrupts the metabolism and hormone regulation in the body. Phosphate diabetes is a congenital form of phosphate loss and is called familial hypophosphatemic rickets designated.
Other diseases can cause the Damage renal tubules and thereby cause too high a loss of phosphate.
The exception to these diseases is a relative phosphate deficiency in premature babies. There may be too much catching-up growth in relation to the low phosphate intake.
Symptoms of rickets
The first symptoms of rickets appear in the second to third month of life.
The children suffer from increased fearfulness, Restlessness, sweat profusely and develop one based on that itchy rash (Miliaria).
From around the 4th month of life the children develop one Frog belly, suffer constipation (Constipation) and kick it first softening of the bones on the skull on (Craniotabes).
In addition, the calcium deficiency leads to a Over-excitability of the muscles up to Muscle spasms. The skull gradually flattens out and the widening of the bone sutures creates the shape of a square skull within a further month.
Also the Widen wrists and ankles increasing (Marfan sign). At the growth plates of the Ribs of Rib cage to step pearl-like swellings on that as rosary are designated.
Of the Tooth eruption occurs later on average and shows Tooth enamel defects on.
Because the rib cage is unusually soft, the muscle pulls the Diaphragm to recoveries (Harrison furrow).
Continue to step Leg curvatures, especially If one on.
These typical signs are only found in childhood. For newly acquired rickets in adulthood, which is called Osteomalacia no typical bone deformations occur. Typically found here dull bone pain and pathological fractures.
Signs of rickets
Typical signs of rickets include restlessness, sweating and a sweat-triggered skin rash as well as increased anxiety in the first three months of life.
In the course of the onset of muscle weakness, a noticeably distended abdomen (Frog belly) caused by relaxation of the abdominal muscles, Flatulence and Tendency to constipation arises.
Then there are the first Signs of bone softening (Craniotabes), which leads to a flattening of the back of the head and in the course to an increased divergence of the cranial sutures with the formation of a square skull.
The lack of calcium can also lead to muscular overexcitability and a tendency to cramp. Like the cranial sutures, the bone-cartilage boundaries of the growth plates float up from the ribs (rosary) and widening deformation of the wrists and ankles occurs.
Another sign of bone deformity is the curvature of the leg (If one), tooth eruption can also be delayed and tooth enamel defective.
diagnosis
The diagnosis is made by the typical bone changes in the X-ray image posed. However, since it is not possible to differentiate between calcium deficiency rickets and phosphate deficiency rickets, the parathyroid hormone must be determined for this. This is increased with a calcium deficiency, with a phosphate deficiency in the normal range. Furthermore, the individual precursors of vitamin D are determined in the laboratory. In this way you can tell exactly whether a classic Vitamin D deficiency- rickets or a vitamin D-dependent form of rickets is present.
X-ray for rickets
In order to be able to diagnose rickets, the anamnese and the clinical examination also the typical laboratory result (Increase in alkaline phosphatase and parathyroid hormone, lower vitamin D levels) and the radiological imaging.
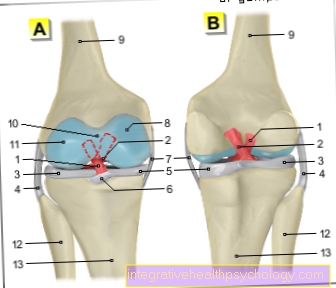
Since a general lack of calcification of the bones and a widening of the growth plates as well as joint and bone deformations are typical signs of rickets, these can best be treated with a conventional one X-ray of the wrist (especially with Vitamin D deficiency-rickets) or the knee joint (especially with Phosphate Deficiency Rickets) to confirm.
The ends of the bones (Epiphyses) appear widened in the X-ray, the bone shafts (Diaphyses) low in calcium and provided with pseudofractures and resorption zones. The transition zones between the end of the bone and the bone shaft (Metaphyses) also show a broadening and appear blurred.
The spongy trabecular system of the bones (substantia spongiosa) is becoming increasingly porous.
therapy
The therapy basically depends on the type of rickets.
Children with a classic vitamin D deficiency rickets get initially Vitamin D and calcium in high doses for 3 weeks. The dosage is then significantly reduced for the next 3 weeks. After that, it is usually sufficient to switch to one calcium-rich diet and adequate sun exposure.
Is there a Type 1 vitamin D-dependent rickets before, this is not enough. Here, the conversion of the preliminary stages is disturbed, so that in addition to high-dose calcium also Calcitriol must be given so that the calcium can be built into the bone. If the bone is replenished with calcium, lifelong therapy with calcitriol is sufficient to maintain the calcium level in the body.
The therapy of Vitamin D-dependent rickets type 2 is, however, much more difficult. Oral intake of calcium and the missing vitamin D precursor (dihydroxy-cholecalciferol) is often insufficient here. Therefore it must be at the beginning of therapy Calcium often in high doses via an infusion are fed. If the body is then saturated with sufficient calcium, it needs calcium continue to be taken orally in very high doses for life taken to maintain calcium levels.
In the Phosphate deficiency rickets must accordingly next Calcitriol phosphate are given. If the cause of the phosphate deficiency is a congenital enzyme disorder, the substitution takes place for life. In the case of a kidney disorder, this must be treated as a priority, if possible, in order to restore the body's own phosphate absorption. The deformed bones in the children usually heal without further therapy, provided that enough calcium and vitamin D are taken in. In the case of severe deformities or phosphate deficiency rickets, operations are often necessary to restore the correct bone position (adjustment osteotomy).
Is rickets curable?
If the rickets is detected in good time and the therapy is initiated early with the diagnosis, most bone misalignments and deformations show regressive, the underlying disease or the one behind the disease hormonal dysregulation however, it cannot be completely cured.
By a temporary or even lifelong Vitamin D or Calcitriol substitution, a possible phosphate substitution and a subsequent prophylaxis in the form of sufficient calcium-containing food intake and sun exposure, the symptoms of rickets can still be contained.
In the most severe rachitic cases, however, the deformations of the legs (bowlegs) can persist, so that in the course of therapy a splinting with orthotics or even a conversion osteosynthesis may be necessary.
Consequences of rickets
The classic consequences of Rachtis disease include multiple bone deformations, especially on the Backbone, of the legs and des Rib cagethat can lead to slight to massive physical restrictions in everyday life. In addition, growth disorders can also occur.
Generalized muscle weakness is also often noticeable in everyday life.
Also a bad one Tooth formation and a restricted immune defense can be counted among the consequences of rickets, whereby the latter can lead to increased infections, which can strongly influence the perception of health.
The increased muscular excitement in the context of rickets can lead to increased muscle cramps or even seizures.
prophylaxis
To prevent rickets, the Daily administration of vitamin D3 in tablet form for babies in the first year of life recommended.
The dose is 500 I.U. per day and is thus well above the actually recommended daily dose of 200 I.U. However, the German Society for Social Pediatrics would like to compensate for any forgotten daily doses. In addition, side effects due to an overdose are very rare and only occur at doses above 2000 I.U. per day. The dosage also applies to breast-fed infants or bottle-fed formula with a specified increased calcium amount. In some cases it is recommended to administer the vitamin D tablet over the second winter.
Summary
Rickets is a relatively common disease caused by a Calcium or phosphate deficiency caused. You can through a decreased intake, increased excretion or one congenital enzyme disorder arise and feed in early childhood Bone deformations and Stunted growth.
Furthermore, the calcium deficiency severe muscle spasms arise. The rickets can be found in the X-ray image diagnose the typical malocclusion of the bones and, with the help of various laboratory parameters, break them down into the classic vitamin D deficiency rickets or a congenital vitamin D dependent rickets.
The same applies to phosphate deficiency rickets, which occurs due to kidney damage or enzyme defects.
Therapy consists in the Substitution of calcium or phosphate and vitamin D3. In addition, in the case of congenital defects, the corresponding hormones and vitamin D precursors must be supplied, sometimes for a lifetime. The deformations of the bones can recede themselves with sufficient calcium intake. In the case of pronounced deformations, an osteotomy must be performed. In Germany, rickets should be prevented by daily oral substitution of vitamin D in the first year of life.