Injury in football
introduction
Football is a dynamic team sport. From a sports medicine point of view, the risk of injury is great. Various characteristics of football are responsible for this:
- Football is a fast-paced sport with lots of quick changes in movement, short sprints, etc., which repeatedly results in short-term peak loads.
- Football is a contact sport with one-on-one fights, header duels, corners, etc .. The risk of injury is great through excessive emotional devotion.
- Football is largely played without protectors.
- Football is played in all weather conditions. The risk of injury is increased in extreme cold, heat and ice.
- In the lower soccer leagues in particular, the space available plays an important role in the risk of injury. An uneven floor, narrow pitch boundaries, hard courts, etc. increase the risk of injury.
Possibilities of injury to the head
Head injuries are not very common. During head-to-head duels, impact injuries can lead to bruises or lacerations. Lacerations of the head look spectacular due to the immediate loss of blood, but are rather harmless in their severity of injury. Lacerations on the skin are sewn up quickly. Despite a large and partly soiled wound, infections are rare.
Adequate protection against tetanus must be ensured. In particular, when training and playing on the cinder pitches, adequate protection against tetanus must be ensured. A booster vaccination should not be given after a graze or laceration.
Broken nose and cheekbone
A slap in the face can cause bony injuries. The broken nose and cheekbone are the most common. Most nasal hernias do not require surgical treatment, provided there is no gross displacement (dislocation) and the olfactory function is not impaired. In any case, an accident doctor should be consulted. If the olfactory sensor is lost, an ENT doctor should be consulted immediately. As an immediate measure, cooling the nose and promoting hemostasis of the neck is suitable.
Malar fractures usually do not have to be operated on. Surgical fracture device (repositioning) and stabilization with metal implants (osteosynthesis) are only necessary in the case of major shifts.
Find out more on our pages on the following topics:
- Broken nose
and - Cheekbone fracture
Possibility of injury to the arms (upper extremity)
The possibilities of injury to the arms (upper extremities) are varied. Most often they arise due to falls.
Falling on the shoulder or the outstretched arm can:
- for ankle joint detonation (ACG detonation)
- a broken collarbone (clavicle fracture)
- for shoulder dislocation (shoulder dislocation)
- a broken arm
- Broken shoulder
or - a tear in the shoulder tendon (rotator cuff tear)
come.
A fall on the wrist can result in a broken spoke (radius fracture).
Kick or fall on the forearm can break this area (forearm fracture).
Shoulder injuries in soccer
Shoulder joint dislocation
When splitting the shoulder joint, the stability ligaments of the shoulder joint (acromio-clavicular joint) tear or tear. If the ligaments are completely ruptured, the lateral end of the collarbone protrudes upwards due to muscle pull (sternocleidomastoid muscle). As a first measure, we recommend immobilizing the affected arm and cooling the shoulder joint. Presentation to the accident doctor (trauma surgeon) on the same day.
Further information can be found at: Ankle joint dislocation
Broken collarbone (clavicle fracture)
A broken collarbone (clavicle fracture) does not always have to be recognized immediately. Usually the collarbone breaks in the middle of the bone shaft, less often at its lateral end and very rarely the sternum - close. There is usually a swelling over the collarbone (clavicle), sometimes a visible misalignment in the sense of a bone step.The affected arm is held in a relieving position. Arm movements, especially attempts to raise the arm, cause severe pain due to the friction between the fractures. Here, too, immediate cooling, immobilization and an early presentation to the accident doctor are recommended.
The soft tissues (nerves, blood vessels) under the collarbone are endangered by an unfavorable fracture shape and a strong fracture displacement. Fractures of the collarbone that have been slightly displaced can be treated conservatively in a rucksack bandage, more complicated fractures and in cases with neurological complications (sensory and movement disorders of the arm), surgical intervention is necessary.
Further information can be found at: Clavicle fracture
Shoulder dislocation (shoulder dislocated)
A shoulder dislocation occurs again and again. Most often the shoulder is dislocated forward and down, i.e. the head of the humerus (humeral head) leaves the socket forwards and downwards, where it gets caught. Immediately after the accident, there is an inability to move the shoulder joint. A large, spherical structure (humerus head) can be felt in the front area of the shoulder, while an empty shoulder joint socket appears in the rear area of the shoulder. A shoulder dislocation can injure nerves and blood vessels.
Therefore, an accident doctor should be consulted immediately, who will adjust the shoulder (repositioned). Partial dislocations (subluxations) of the shoulder are possible. The humerus head does not leave the shoulder joint completely. In these cases, the head of the humerus can snap back spontaneously into its socket through an involuntary arm movement of the injured person.
After the doctor has successfully repositioned the shoulder, a magnetic resonance imaging (MRI) examination of the shoulder is recommended in order to detect any accompanying damage to the shoulder joint. This includes the rotator cuff tear and the tear off of the anterior shoulder joint lip (labrum).
Further information can be found at: Shoulder dislocation
Rotator cuff tear
A rotator cuff tear is often the result of a shoulder dislocation. The rotator cuff refers to the muscle / tendon sheath of the muscles involved in the rotation of the shoulder joint. The supraspinatus muscle is mostly affected. A rotator cuff tear alone is also possible, albeit less often and then mostly affects a previously damaged (worn, degenerative) tendon.
Surgical restoration of the rotator cuff should be sought, because the tendons, in addition to their movement function, have an important function for centering the humerus head in the joint socket.
For more information, see: Shoulder tendon tear
Upper arm injury
Upper arm fracture
Shoulder and upper arm fractures are very rare injuries. If the impact trauma is very severe, the shoulder blade (scapula) can break. Upper arm fractures (humerus fractures) can affect the upper arm head, the upper arm shaft and the humerus rolls (condyles). Surgical care is usually necessary.
Read more on this topic at: Upper arm fracture
Forearm injury
Broken spoke
A radius fracture (spoke fracture) at a typical location (Loco typico) typically occurs when the player tries to catch a fall with his arm. Depending on the position of the wrist on impact, different fracture forms result. A shot in the flexed wrist can also cause a wrist fracture. If a broken wrist is suspected, the wrist should be cooled and the wrist immobilized. Surgical care will often be necessary.
A complete forearm fracture can often be recognized by the gross misalignment of the forearm. In both cases, an accident doctor should be consulted immediately.
For more information, see: Broken spoke
Possibilities of Injury to the Lower Limb
Injuries to the lower extremities are the most common in soccer. On the one hand, it is an intensive running sport, on the other hand, the play equipment is promoted by the leg and foot activity. While in the area of the upper extremity it was predominantly the traumatic falls that led to the injury, in the area of the lower extremity there are also causes of injuries other than falls.
Bruise and bruise:
One of the more minor injuries to the lower extremity is a bruise, which manifests itself as a local swelling and a painful bruise. This injury, also popularly known as the "horse kiss", is caused by external force, such as a hard kick on the thigh, knee, or calf.
Read more on the topic: Horse kiss
Muscle injuries:
Torn muscles and torn muscles are probably the most common injuries in football and cause the game to be stopped immediately. Cold or tired muscles, but also not very flexible muscles, are particularly at risk of injury. As a result, the football player typically suffers from strains or torn muscle fibers at the beginning of the game, when his muscles are poorly warmed up, or at the end of the game, when the muscles become tired and the individual movements are less coordinated. Another reason for injury is the lack of flexibility of the tendons and muscles in footballers, due to one-sided muscles on the one hand and shortened muscles on the other.
The back thigh muscles (hamstring muscles) are typically shortened muscles in footballers. During a fast sprint, these muscles tend to be pulled. The player experiences a sudden sharp pain in the back of the thigh, followed by some sort of cramping sensation. Stretching, such as a muscle spasm or heat treatment, should definitely be avoided. Rather, as with all muscle injuries, the rules of the PECH scheme apply to the initial treatment (break / ice / compression / elevation).
Another typical muscle injury is adductor strain, i.e. the muscle group that is responsible for bringing the leg closer to the body. Injuries of this type occur e.g. by spreading the leg strongly to the side, as when tackling, or if the standing leg suddenly slips away when changing direction. Pain occurs in the area of the inner thigh or in the groin, where the adductors originate.
A muscle injury that occurs during the ball shot is the strain of the rectus femoris muscle on the front of the thigh. This muscle, which is well developed in footballers, suddenly becomes tense when shooting. With cold muscles and less trained or tired muscles, this can lead to injuries. The pain localization is on the front of the thigh.
Overall, it is very difficult to distinguish between a slight or severe muscle strain and a muscle fiber tear. A torn muscle fiber does not necessarily lead to a bruise (hematoma) in the muscles. The examination methods available in the doctor's office, especially ultrasound (sonography), cannot detect a muscle fiber tear due to the lack of image resolution. An indication of a ruptured muscle fiber is a bleeding into the muscular valleys, which usually does not occur with a mere muscle strain. In the next larger lesion, the muscle bundle tear, a bruise can regularly be detected. It is easy to diagnose a complete muscle tear, which is already noticeable when looking at it and when feeling it through a strong muscle gap in the muscle network. The function of the muscle concerned is suspended.
For more information, see: Torn muscle fiber
Knee injuries
The knee is the footballer's joint that is most often injured. Soccer is a sport that puts a lot of strain on the knees and involves a lot of non-physiological rotational movements under high stress.
Classic injury patterns are the meniscus tear, cruciate ligament tear or a collateral ligament injury.
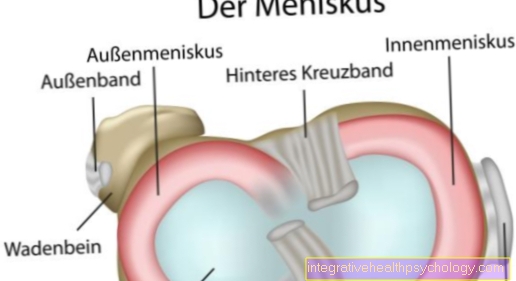
Meniscus tear
The inner meniscus is usually affected by a meniscus tear (meniscus rupture). It is particularly prone to injury due to the relatively rigid (rigid) attachment in the knee joint compared to the outer meniscus. This means that he is less able to avoid peak loads. A distinction is also made between degenerative meniscus tears, which are based on previous damage to the meniscus and which can occur without an accident, from suddenly occurring meniscus tears in young, healthy athletes without signs of degeneration. The accident usually results from a sudden external turning movement of the knee joint with slight flexion and the lower leg fixed. This results in a strong pressure load with simultaneous shear load on the inner meniscus. The footballer feels a sudden, stabbing pain in the knee joint. The knee can swell a lot. Most of the young athletes are more likely to have a basket handle tear form in the meniscus, which can pinch parts of the meniscus in the knee joint. In this case, the knee joint can no longer be fully extended and flexed. The initial treatment is based on the PECH scheme. In the clinic it is sometimes possible to use mobilization techniques to free the meniscus and thus to alleviate the extremely painful clinical picture. A partial removal of the meniscus or a meniscus suturing can be considered therapeutically.
Further information can be found at:
- Meniscal tear
- Meniscal surgery
Cruciate ligament tear
The cruciate ligament tear is a severe knee joint injury with long-term consequences for the knee joint. The course of the injury is similar to the meniscus tear described above. In fact, simultaneous injuries to the anterior cruciate ligament and medial meniscus are often found. If the inner ligament is also injured at the same time, this is called an unhappy triad. ly the anterior cruciate ligament tears. The knee joint almost always swells up a lot and is painful to strain. The mobility of the knee joint is limited by the bruise. The typical anterior knee instability usually cannot be determined in the early phase of the injury due to painful muscle tension and effusion. The therapy is operative. We and most experts do not share the general opinion that is often still propagated that one does not need to operate on an anterior cruciate ligament rupture with good muscular stabilization. An individual decision must always be made, taking into account all the factors involved.
Further information can be found at:
- anterior cruciate ligament tear
- posterior cruciate ligament tear
- Cruciate ligament overstretched
Collateral ligament injury
Collateral ligament injuries can occur in isolation or together with cruciate ligament and meniscus injuries. Often it is harmless collateral ligament strains that heal after 3-6 weeks and do not require any special treatment other than a break in sports. Collateral ligament injuries result from lateral stress on the knee joint. In the case of an inner ligament injury, the stress occurs from the outside, in the case of an outer ligament tear from the inside.
An isolated rupture of the inner ligament can be treated conservatively in a knee-joint orthosis with lateral support; surgery is more often recommended for the rarer outer ligament rupture.
Ankle injuries
Outer ligament tear
An uneven playing field surface can be the cause of a torn outer ligament (fibular ligament rupture) of the ankle due to the classic ankle injury. Depending on the force applied, the 3 outer ligaments (fibular ligament apparatus) are initially stretched, later they tear. The anterior outer ligament (ligamentum fibulotalare anterius) is most often affected by a tear. This stretches from the outer ankle (fibula) to the anterior part of the ankle bone (talus). In the early stages of the injury, the ankle swells a lot. The severity of the injury cannot be reliably estimated. The initial treatment is again based on the PECH scheme. The therapy is mostly conservative in an air cushion splint for about 6 weeks.
For more information, see: Torn ligament
Broken bone
A very severe twisting of an ankle or a direct kick on the fibula can lead to a fracture of the outer ankle. If there is no visible bone deformity, the external aspect is similar to that of the ligament tear. However, the pain point is less below or in front of the outer ankle than it is on or above the outer ankle. The therapy is mostly surgical with setting up the fracture and metal stabilization (osteosynthesis).
Further information can be found at: Outer ankle fracture
An injury that is easily overlooked is the fracture of the 5th metatarsal, usually at the base of the 5th metatarsal (5-base metatarsal fracture). A twisting is also the cause. The pain point, however, is more in the area of the lateral back of the foot or the outer edge of the foot. Therapy can be surgical or conservative. If the fragments are removed from each other (dislocation), surgery should be carried out, otherwise the therapy can be carried out in a plaster cast alone.
Further information can be found at: Fracture of the 5th metatarsal
Achilles tendon tear
It is not uncommon for older amateur footballers to suffer from a ruptured Achilles tendon. There is usually no accident. Patients report a sudden pain in the calf when walking, accompanied by a bang that is said to be like a lash. A torn muscle fiber of the calf muscles must also be considered in the differential diagnosis. The therapy is mostly surgical with suturing of the Achilles tendon.
Read more on this topic at:
- Achilles tendon tear
and - Achilles tendon
Impingement ankle
A more chronic footballer's disease is the formation of tibial edge osteophytes (footballer's ankle) on the front of the ankle-forming tibia. These are bony edges (attachments, osteophytes) that have arisen from microtraumatisation of the bone through years of cocking.
When the foot rolls, these edges can hit and lead to chronic anterior ankle pain. If the symptoms are symptomatic, the therapy consists in the arthroscopic removal of these edges.
Note
In the event of unclear complaints, we would like to contact our Diagnostic refer. On the basis of your complaints and symptoms, you can use our diagnostic tool to diagnose your disease.