Amputation heights
Determination of the amputation level

The previously made rigid determination of the amputation level by so-called amputation schemes with division into valuable, dispensable and obstructive extremity sections is now outdated and should be rejected.
For the various amputation heights and forms, the extent to which the stump is capable of bearing loads and is suitable for receiving a prosthesis must be observed.
Amputation of hand, elbow and shoulder
On the upper extremity, the amputation through the shoulder girdle, i.e. between the shoulder blade (scapula) and the chest (thorax), is the highest point of a possible decrease.
The cause here is usually a malignant tumor and causes considerable cosmetic and functional damage. The consequences of a shoulder disarticulation, i.e. an upper arm amputation from the shoulder joint, are similar.
In the case of an amputation of the humerus, care must be taken to ensure that there is enough space for an artificial elbow joint at the amputation height.
Disarticulations (amputations) in the elbow joint itself are difficult, as protruding bone parts result, which can cause painful pressure points in the prosthesis shaft.
The hands are capable of complex fine motor movements and are extremely important for daily life and work, so that an amputation leads to considerable impairment. In the area of the hand, in addition to resilience, the length of the stump, the sensitivity, the mobility of the joints and the possible forms of gripping must be taken into account. Even the loss of a thumb makes gripping processes almost impossible.
Read on below: Amputation of a finger
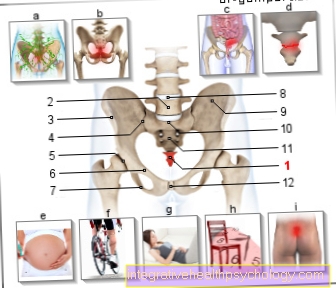
Amputation of the leg, foot, lower leg
In the area of the lower extremity, the form of loading is of course different from that of the upper extremity.
In the case of metatarsal and tarsal amputations, care must be taken that the skin of the sole of the foot, which is particularly stable, and the fat layer underneath it, as well as the short foot flexor muscles, are used to cover the residual limb and that the scars lie on the stretch side, i.e. on the back of the foot, outside the stress zone, as otherwise painful pressure points can arise.
In the case of diabetic foot syndrome with necrosis (gangrene) or diabetic microangiopathy (disease of the smaller vessels), border zone amputations are carried out, which can be demarcated on anatomically defined lines on the metatarsus.
In the case of amputations of the lower leg, the entire tibia (tibia) and fibula can usually be preserved and a separation can be made just above the ankle joint (Syme amputation), but this stump can only be prosthetically treated with difficulty and cannot always carry unrestricted weight.
More often, however, an amputation is performed in the area between the upper and middle third of the lower leg. The stump can be supplied with a myoplasty, i.e. the muscles that functionally act as opponents (antagonists) are connected to one another around the end of the bone.
But also a muscle-skin flap folded from the back (dorsal) to the front (ventral) is capable of supplying the residual limb.
The disarticulation of the knee joint, which was previously rejected because of its sparse stump coverage without muscles, is now performed more and more frequently in PAD (peripheral arterial occlusive disease) patients. The advantages lie in the length of the stump (lever arm) and the strength (preserved thigh muscles).
Find out more at: Thigh amputation, lower leg prosthesis
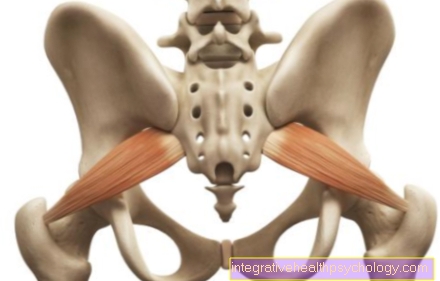
At the Vascular patients the amputation level depends on the blood flow to the Musculature. So it may be that a thigh amputation has to be performed. The optimal height for this is in the middle of the Thighbone. The bone stump must be significantly shortened compared to the skin soft tissue layer so that the opposing (antagonistic) muscles can be sutured over the thigh bone (femur).
In this so-called myoplasty, the muscles must first be fixed to the bone (myodesis), after which they can be sutured together. This maintains good muscle tension and activity and ensures good padding.
The Risk of neuroma formation is mainly in the nerves supplying the thigh (Sciatic nerve), so this must be tied (ligated) well above the amputation site.
A Hip joint disarticulation is a far more difficult procedure with large soft tissue wound and high mortality (death of the patient). It should only be used in the case of the most severe infections or tumors.