Aortic aneurysm
definition
Under a Aortic aneurysm one understands a bulging of the vessel wall or the Vessel walls. At least one layer must be affected to meet the definition.

Symptoms
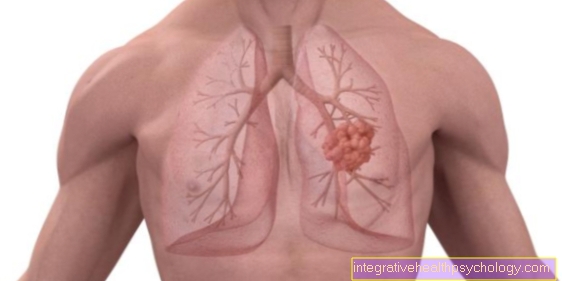
An aortic aneurysm is a pathological enlargement of the main artery (aorta). It occurs either in the chest or in the abdomen. Initially, there are no symptoms in the abdominal cavity, making it difficult to identify the aneurysm at an early stage. The unspecific symptoms can easily be confused with other illnesses, such as a heart attack. When it increases in size, it presses on the surrounding organs and can lead to discomfort.
From a certain size it is possible in some cases to feel the aneurysm pulsating on the abdomen. It can also lead to diffuse back pain. An aortic aneurysm in the chest causes symptoms such as coughing, hoarseness, chest pain, shortness of breath and difficulty swallowing.
In the case of a rupture, there is very severe pain in the abdominal or chest area, radiating to the back. The subsequent high blood loss leads to circulatory collapse with shock symptoms and represents an acutely life-threatening situation.
More on this: Symptoms of an aortic aneurysm
What pain does an aortic aneurysm cause?
An aneurysm in the abdomen does not initially cause any symptoms. As it increases in size, it can cause pain in the lower abdomen that can spread to the legs. Diffuse back pain is also possible. In the chest area, aneurysm causes chest pain. Swallowing disorders and shortness of breath can also occur. A rupture of the aneurysm causes extremely severe pain in the chest or abdomen, depending on the location.
hoarseness
Hoarseness can be a symptom of an aortic aneurysm in the chest. Above a certain size, the aneurysm can affect the recurrent laryngeal nerve. This nerve innervates a large part of the muscles in the larynx. If the aneurysm presses on this nerve, recurrent palsy occurs, which then results in hoarseness.
Read more about this: Vocal cord paralysis
diagnosis
First and foremost is the patient survey (anamnese) and the clinical examination. When taking the anamnesis, it is particularly important to inquire about any accompanying illnesses. If the patient claims to have coronary artery disease, suspicion of an aortic aneurysm must be considered (55% of cases). Other diseases that are often found as concomitant diseases are high blood pressure and arterial occlusive disease, heart failure and diabetes mellitus.
During the physical exam, the doctor must examine the abdomen more closely. Touching (Palpation) and listening to the abdomen with a stethoscope (ausculation) can provide indications of an abdominal aortic aneurysm (typical: buzzing, hissing, pulsing).
If an aortic aneurysm is suspected, an ultrasound examination must be performed. In many cases a bulging of the aorta can be seen in this. A special setting (color Doppler) allows the doctor to control the blood flow in the vessel by color. Unnaturally large eddies would also indicate an aneurysm. The aortic diameter is also important for the ultrasound examination. If a normal value of 2.5 cm is exceeded, one speaks of an aortic ectasia (2.5 cm-3 cm). A diameter over 3 cm is then called an aneurysm. Also, during the ultrasound examination, the search for free fluid should not be forgotten, the presence of which could indicate an already ruptured aneurysm.
With the help of a computed tomography (CT), which in this case should be performed with a contrast medium, an aneurysm can also be made visible. In the CT cross-sectional image, one usually sees a crescent-shaped protrusion or a so-called "mirror egg image", which is missing in the other areas of the vessel. Coagulated blood (thrombotic material) that has already formed at the aneurysm can also be made visible in the CT image. It is also important to check the outgoing vessels (e.g. kidney vessels), as the blood supply to the adjacent organs must be guaranteed. Alternatively, magnetic resonance imaging (MRI) be performed. However, this takes much longer than CT and is more of the second choice, especially in emergency situations (ruptured aortic aneurysm). Further arteries must be examined for aneurysm formation. In addition to the aortic aneurysm, many patients also have renal artery and carotid aneurysms. The diagnostic agent of choice here is the ultrasound examination.
treatment
There are basically two different ways to treat an aortic aneurysm. In the case of smaller aneurysms, it is better to wait and do regular ultrasound checks. In addition, risk factors that favor aneurysm or its rupture should be treated or avoided. This includes keeping the blood pressure in the normal range of around 120/80, in some cases also with antihypertensive drugs. Diabetes and lipid metabolism disorders also need treatment.
For larger aneurysms in the abdomen, either open surgery is available, in which the enlarged piece of the aorta is removed and replaced with a prosthesis. There is also the possibility of introducing a kind of stent over the artery in the groin and placing it in the place of the aneurysm. As a result, the blood no longer flows into the aneurysm but past it via the stent. Open surgery is usually performed on the chest. If the aneurysm is close to the heart, the aortic valve may also need to be replaced.
also read:
- Artificial heart valves
- Therapy of an aortic aneurysm
When do you need an operation?
If there is an aneurysm in the chest area, surgery should be performed from a size of 55 mm. If there is a disease of the connective tissue (e.g. Ehlers-Danlos syndrome or Marfan syndrome) the limit is 50 mm.
Surgery is indicated even with rapid growth of more than 2 mm per year. An abdominal aortic aneurysm should be operated on when the size is 60 mm. Further indications are a rapid increase in size of more than 0.5 cm in three months, symptoms due to the aortic aneurysm and a high risk of a rupture e.g. with poorly controllable high blood pressure.
Aortic prosthesis
An aortic prosthesis is a tissue tube that is used in the treatment of the aortic aneurysm. If the aneurysm exceeds a certain size, surgery should be performed, because the larger the diameter, the greater the risk of rupture. The prosthesis can be inserted in two ways. On the one hand, the affected part of the aorta is replaced by the prosthesis during an operation, on the other hand there is a minimally invasive method using a catheter. Here, the prosthesis is folded up and pushed through a vessel to the affected area. Here it unfolds and thus removes the aneurysm from the bloodstream.
Complication: rupture of the aneurysm
The rupture of an aortic aneurysm is a life-threatening complication. Once a bulging of the vessel wall has formed, it usually continues to expand. With a diameter of more than 55 mm in the chest area and more than 60 mm in the abdomen, the risk of a rupture is particularly high. The bursting of the aneurysm leads to extremely severe pain in the abdomen or chest, often accompanied by nausea and nausea. Internal bleeding occurs, in which the person concerned can lose very large amounts of blood within a very short time. The consequence is circulatory shock and, in most cases, death.
Further information on this: Aortic rupture
Chances of survival
The chances of survival from a rupture of the aortic aneurysm are poor. If a rupture occurs outside of a hospital, half of those affected die on the way to the hospital. A quarter can then no longer be treated successfully in the clinic because the blood loss is already too great. 40% of the patients who undergo surgery do not survive. Only in a few cases is there a real chance of survival, as the time for a successful intervention is very short. In contrast, an aortic aneurysm that is identified and treated at an early stage has a good prognosis.
Does an aortic aneurysm have a reduced life expectancy?
Life expectancy with an aortic aneurysm depends on many factors. On the one hand, it is important that the aneurysm is discovered and treated in good time. If this happens too late, there is a risk of rupture, which in most cases results in death. After a successful procedure, the risk of rupture is very low. However, life expectancy now depends on the underlying disease such as Atherosclerosis. Because the operation "repairs" the aneurysm, but does not treat the cause. The arteriosclerosis therefore persists and can lead to further diseases.
causes
In most cases, the cause is high blood pressure (hypertension) and the resulting hardening of the arteries (arteriosclerosis). In particular, undetected and untreated hypertension that persists over a long period of time is responsible for the formation of an aortic aneurysm.
Another cause of the aortic aneurysm can be trauma from a car accident (acceleration injury) or a doctor's vascular puncture. In general, one can say that previous vascular injuries of any kind can lead to an aortic aneurysm. Inflammatory causes, such as inflammation of the arteries
(Arteritis), bacterial infections (syphilis) or fungal infections are a rare cause. Very rarely, an aortic aneurysm results from what is known as cystic median necrosis or the rare Kawasaki syndrome.
If the aorta constricts for whatever reason, the area behind the constriction usually begins to widen. An aneurysm develops.
An aortic aneurysm can also be congenital. There are some diseases that affect the organism's collagen system. Since collagen is also present in the vessel walls, a disruption in collagen synthesis leads to instability, which can result in an aneurysm. Mention should be made here of the so-called Ehlers-Danlos syndrome (those affected usually notice an unnatural ability to overstretch the joints). Marfan's syndrome is a malformation syndrome of the mesenchyme. This often results in an inability to close the heart valves (mitral insufficiency) and / or an aortic aneurysm.
Furthermore, one assumes a hereditary component that promotes the formation of aortic aneurysms.
Read more on the topic: Atheromatosis
Classification
In principle, one can differentiate between three types of aortic aneurysm.
- Aneurysm verum,
- Aneurysm dissecans and that
- Aneurysm spurium.
1. The verum aneurysm is also known as the true aneurysm. It is a sack-like or spindle-shaped overstretching and sagging of all three wall layers (the so-called intima, media and adventitia).
2. At Aneurysm dissecans there is only an intimal tear. The blood gets through the tear into the inner vessel wall and splits it (dissection, rooting bleeding). This creates a double lumen that may can extend from the main artery (aorta) of the chest to the abdominal aorta. This leads to an overstretching of the outer vessel wall (Adventitia), which may can press the outgoing vessels. In this case, certain areas of the body are no longer supplied with blood (descending ischemia syndrome). The blood that has got between the layers can possibly re-enter the regular vessel through a window. There is also the Aneurysm dissecans the possibility of self-healing. A later tear is not excluded and must be feared.
Read more on this topic: Aortic dissection
3. That Aneurysm spurium is also called a false aneurysm (False aneurysm) designated. Blood leaks from the blood vessel through a leak in the artery wall and forms a bruise in front of it (hematoma). After a while, a capsule of connective tissue forms around the hemorrhage, which then emerges as a bulge. Since this is not the vessel wall, as is the case with the other aneurysms, it is also referred to as a false aneurysm.
In addition to this classification, the aortic aneurysms are also classified according to their height location on the aorta. The main artery (aorta) leading from the heart, which merges into the abdominal aorta via the aortic arch, is divided into 5 segments. According to DeBakey, a type 1 aortic aneurysm can affect the entire aorta. Aortic aneurysm type 2 is only available to the Ascending aorta limited. Type 3 aortic aneurysm affects the area below the left subclavian.
Another classification of the aortic aneurysm can be made according to Stanford. Only two groups are distinguished here. While type A is on the aortic arch and the ascending aorta, type B is on the descending aorta behind the exit of the Subclavian artery localized.
Finally, the aneurysms can also be classified according to their shape. The Sacciform aneurysm is rather sack-shaped, that Fusiform aneurysm rather fusiform and the saccifusiform aneurysm is mixed. A boat-shaped shape would be called a Cuneiform aneurysm and a serpentine, which consists of different aneurysms (Aneurysmosis) as Serpentine aneurysm describe.
Some of the potential complications include aortic dissection, a tear in the inner wall of the aorta. This is accompanied by sudden, stabbing pain of the greatest intensity.
Why does the aneurysm occur especially in the abdomen?
An aortic aneurysm most commonly occurs in the abdomen. In 90% of cases, it forms below the renal artery. The exact reason for this has not yet been fully clarified. It could be that the structures and organs surrounding the aorta favor a bulging of the aortic wall at this point, or that the pressure in the vessel is particularly high due to certain factors. Another reason are probably processes that take place at the cellular level, but which have not yet been fully understood.
Can you do sports with an aortic aneurysm, and what kind of exercise?
In principle, exercise is possible with an aortic aneurysm. However, the diameter of the aneurysm and the underlying disease are very important. So it must be decided individually for each patient. In general, it can be said that if you have an aortic aneurysm, you should avoid exercise that causes blood pressure to rise sharply. One example of this is weight training. An increase in blood pressure increases the pressure on the aortic wall and thus promotes a life-threatening rupture. However, aerobic endurance sports such as Nordic walking are recommended.
Epidemiology
Men are predominantly affected by the aortic aneurysm (ratio to women 6: 1). The maximum age is between 65 and 75 years of age. Since there is no preventive medical check-up in the sense of an aortic aneurysm, a relatively high number of unreported cases can be assumed, even among younger patients. In 10% of elderly patients who are under one high blood pressure an aortic aneurysm is discovered.
MRI of the aorta
When planning the therapy of the aortic aneurysm, it is important to have an imaging method to assess the aneurysm and the vessel wall. Either CT or MRI with contrast agent is used for this. MRI is superior to CT because it can better show the structure of the vessel wall and there is no radiation exposure for the patient, but because of the greater time required, it cannot be used in emergencies. Since magnetic radiation is used in MRI, it cannot be used on patients with cardiac pacemakers or metallic stents.
Summary
As Aneurysm one describes a bulging of the vessel wall. A distinction is made between the aneurysm verum (real aneurysm), in which the entire vascular wall is everted, the aneurysm dissecans, in which there is bleeding between the two vascular layers, and the aneurysm spurium in which all wall layers rupture with simultaneous bleeding into the surrounding area Tissue comes.
In this type of aneurysm, a covering later forms around the bleeding, which in turn can exert pressure and dysfunction on the surrounding organs.
In addition to various inherited disorders of collagen and connective tissue synthesis, the main causes of an aortic aneurysm are high blood pressure and arteriosclerosis. For this reason, optimal blood pressure adjustment is essential in these patients. An aneurysm is usually diagnosed by ultrasound examination of the blood vessels.
The exact location and further information is provided by a Computed tomography (CT) or. Magnetic resonance imaging (MRI). 30% of aneurysms cause no discomfort and are detected, if at all, by a random ultrasound examination. 45% cause back and flank pain.
Urgent surgery is indicated if the aortic aneurysm ruptures or has an aneurysm diameter of more than 5 cm. The chest is opened, the main artery is clamped from the bloodstream and either after the aneurysm has been removed, the open area is sutured or a plastic-coated tube (stent) is inserted.
All aortic aneurysms that are smaller than 4 cm and do not trigger any symptoms should be closely monitored by ultrasound controls. An increase in size must not exceed 0.4 cm per year. If this is the case, surgery is also indicated.
Without treatment, 50% of asymptomatic aneurysms will tear within the next 10 years. Symptomatic aneurysms tear on average after 1-2 years (90%). In the case of a planned operation, 4-7% of the patients die, in the case of emergency surgery up to 50-90%.
Aortic aneurysm is a serious clinical picture, the chances of success of a cure has increased significantly in recent years thanks to better materials and surgical procedures.