Liver resection
introduction
Liver resections are surgical procedures in which parts of the liver are removed. This is possible because the liver - unlike other organs - has the ability to regenerate itself to a certain extent. It is possible that the liver will regenerate up to 80% of its original size. This means that the liver can grow back after the procedure if too much liver tissue has not been removed. It is even possible to remove half of the liver, in which case it is called one Hemihepatectomy. The entire liver can only be removed if a suitable liver transplant is available for the patient, because the liver is a vital metabolic organ in our body.

Liver resections are performed in different cases carried out. Liver cancers and the Bile ducts or Metastases in the liver from tumors of other organs can make a resection necessary. Also Abscesses of the liver or Cysts If the findings are large, they may result in a liver resection. In addition, there is an infection caused by the Tapeworm Echinococcus multiloculariswhich may require a liver resection.
Liver resection procedure
A (partial) liver resection can be performed either through open surgery or minimally invasive through a laparoscopy. Both types of surgery require an inpatient stay for several days to weeks and general anesthesia.
In the open procedure, a larger abdominal incision is made to open the abdominal cavity; in the minimally invasive procedure, surgical tools and a camera are introduced through several small incisions. Before the actual resection, an ultrasound probe is often placed directly on the liver tissue and the entire organ is displayed once. As a result, further abnormalities can be identified which could not be seen in the imaging diagnostics carried out previously. If this examination does not reveal any reasons against the planned intervention, the part of the liver that is to be removed is exposed and exposed. It is particularly important to expose the supplying blood vessels, which must be closed by means of clips or threads in order to avoid major bleeding. The liver part to be resected is then detached. This can be done either with targeted current surges, a laser probe or conventional cutting tools. As a rule, the resection surface is then obliterated in order to prevent secondary bleeding and leakage of bile. Before the operation is completed, the abdominal cavity is rinsed. Finally, the abdominal wall is closed again. Often, but not always, there is a scheduled surveillance stay in the intensive care unit before the patient can be transferred to the normal ward for a few days and then discharged.
Indications for a liver resection
Indications for a partial liver resection can be both benign and malignant diseases of the liver. The benign diseases include, for example, encapsulated purulent inflammations (liver abscesses) or an infection with dog tapeworms (echinococcal cysts). Among the malignant diseases for which a partial liver resection is indicated, liver cancer (hepatocellular carcinoma = HCC) should be mentioned first. If the disease is recognized in time or if the patient's circumstances allow, surgical removal of the tumor can, in the best case, cure it. Another indication for a partial liver resection is when another tumor, such as colon cancer, has spread to the liver and the metastases can be removed by the procedure.
Liver cancer
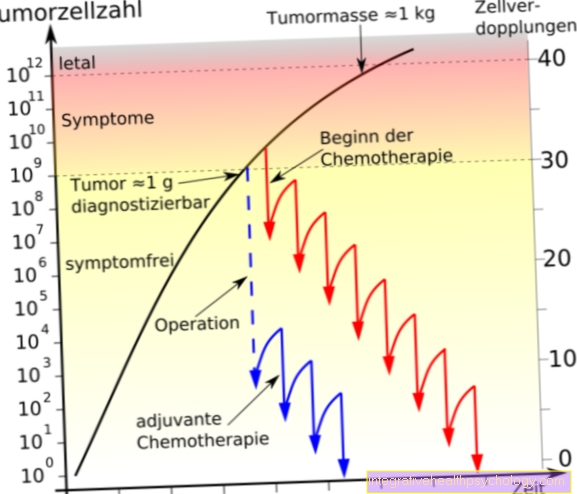
The decision as to how a tumor disease of the liver is or can be treated depends on the size of the finding. There are many different ways to cure liver cancer, the most common type of liver tumor, but hepatocellular carcinoma does not respond well to chemotherapy drugs. Therefore, the surgical approach is usually followed.
A partial liver resection can only be performed if the remainder of the liver is still functional, i.e. if there is no cirrhosis of the liver. This is rarely the case. If the tumor can be removed without the need to transplant a new liver, it is important that the tumor be completely removed. To ensure this, not only the tumor, but also part of the surrounding healthy tissue should be removed so that no new tumors can grow.
Read more on the topic Liver cancer therapy
Metastases
Metastases are not tumors in their own right. If metastases appear in the liver, they would not be called a liver tumor. They are tumor cells from tumors in other organs that were transported to the liver via the bloodstream and where they have grown into so-called metastases.
Most commonly affected by liver metastases are patients with colon cancer, breast cancer, lung cancer, gastric and esophageal cancer. They occur in advanced stages of the tumor disease. Chemotherapy can initially prevent cancer cells from spreading throughout the body from the original tumor.
Liver resection is usually the therapy of choice for the local therapy of metastases in the liver from other organs. A combination of systemic therapy (chemotherapy) and local liver resection is often used.
Duration of the operative liver resection & hospital stay
An exact Duration of the operation is difficult to determine in advance. The duration varies depending on the type of procedure chosen (open vs. laparoscopic), the complexity of the resection, and the occurrence of complications.
A liver resection can do so between three and seven hours last. After the operation you will mostly be for 24 hours in the intensive care unit housed a precautionary measure to prevent the postoperatively Vcheck ital functions optimally and to be able to respond best to possible complications after the operation.
The Length of hospital stay lies between four and eight days, In the event of complications, this length of stay can be extended. Overall, it depends very much on the individual circumstances of the patient. A follow-up treatment, so one Rehab, is generally not provided.
Complications
Every surgical procedure carries risks. First, complications can arise during the anesthesia occur, such as allergies to the anesthetics used.
Furthermore, the surgical intervention Soft tissue, annoy and Blood vessels be harmed. Damage to blood vessels can cause bleeding. As a rule, the surgeon can quickly control and stop the bleeding no life-threatening threat for the patient. In rare cases, however, extensive bleeding can occur and a transfusion of foreign or autologous blood that was previously donated is required.
Blood transfusions are often necessary for liver resections because the liver is an organ with a very high blood supply. Blood transfusions can cause infections that harm the patient. In extremely rare cases, infectious diseases can be caused by blood transfusions, for example hepatitis be transmitted. Fortunately, with strict controls on blood products, these transmissions have become very rare.
It can also be caused by the surgery itself Infections come. The causes of these infections can be very different: accumulations of residual blood (Hematomas) can catch fire, but it can also lead to Injury to surrounding organslike that Intestines causing bacteria to escape and infect the abdomen. This also makes surgical treatment of the intestine necessary. Of the Bile leakage Getting out of the bile ducts during or after surgery is also problematic as it becomes too Inflammation of the peritoneum can lead, which makes a renewed intervention necessary. Furthermore, it can lead to the formation of Fistulas which rarely cause problems in the course of the process. Injuries or obstructions to the biliary tract can have the consequence that the bile cannot drain properly and builds up. It is possible for it to be Jaundice (Jaundice) is coming. In this case, another intervention is necessary to allow the bile to drain.
In the case of a resection of a tumor, it can be Carry-over of tumor cells come, this is however very rare the case because the surgeons are very careful to prevent this.
In addition, there are other possible complications that can occur with all surgical interventions: the risk of thrombosis or embolismthat the lungs (Pulmonary embolism), the heart (heart attack) or the brain (stroke).
It can too Wound healing disorders come in the seam area.
It may also be necessary to change the surgical procedure in order to avoid or resolve complications. To minimize the risks and complications of this procedure, there are several future-oriented procedures, such as minimally invasive surgery or CT and MRT-based procedures.
Risks
As with any surgical procedure, there are general risks associated with resections of the liver, such as damage to surrounding organs, blood vessels or nerve tracts. There may also be blood loss, which requires the transfusion of blood units. This is often necessary, especially with extensive liver resections. In addition, despite all hygienic measures, inflammation can occur, which can extend to peritonitis and blood poisoning. In the worst case scenario, these risks can be life-threatening. In addition, bleeding or wound healing disorders can occur after the operation. In rare cases, it is necessary to operate again. Added to this are the risks of the general anesthesia required for this procedure, such as an allergic reaction to one of the substances administered. A special risk associated with resection of liver tissue is the leakage of bile from the resection surface or unclosed bile ducts, which can subsequently lead to life-threatening peritonitis and also occasionally require another operation. In addition, the draining biliary tract can be injured during the liver resection in such a way that the drainage is disrupted and the bile is backed up. This manifests itself among other things by a yellow discoloration of the eyes and skin (jaundice = “jaundice”).
Aftercare
Often no special follow-up treatment is required after an uncomplicated liver resection. The necessary measures are mainly based on the disease for which the operation was performed. In the case of a benign disease such as a liver abscess (encapsulated purulent inflammatory focus), the procedure can usually completely cure it. If a malignant disease such as colon cancer is present and metastases (“daughter tumors”) of the underlying tumor were removed during liver resection, chemotherapy may also be necessary. Follow-up examinations, for example using ultrasound, are usually required after a liver resection. When and how often these are necessary, the doctor also determines depending on the disease.
Diet after liver resection
After a complication-free partial liver resection, nothing special needs to be considered in terms of nutrition. As a rule, the liver tissue left in place can fulfill the tasks of the organ without restriction. For example, a particularly high-protein diet may only be indicated if the liver function is impaired anyway. In individual cases, however, the attending physician will explain whether certain dietary issues should be observed after a partial liver resection.
What is the Pringle Maneuver?
The Pringle maneuver describes a surgical step in which the blood flow to the liver is blocked with a hemostat. The clamp is placed on the so-called hepatoduodenal ligament, which contains the hepatic artery (Arteria hepatica propria) and the portal vein (Vena porta) as blood-carrying vessels. In addition, the main bile duct (ductus choledochus) runs in the ligamentum hepatoduodenla. The latter, however, is left out when unclamping so that it is not injured. As a result of the Pringle maneuver, the liver is no longer supplied with blood and the liver operation can be carried out with significantly less blood loss. If the liver is not previously damaged, the maneuver is usually tolerated for up to 60 minutes without any consequential damage.