Stomach cancer
Synonyms
Medical: gastric cancer
Gastric tumor, gastric Ca, gastric adenocarcinoma, cardiac tumor
definition
Of the Gastric cancer (gastric cancer) is the fifth most common cancer in women and the fourth most common in men. The gastric carcinoma is a malignant, uncontrollably growing tumor that is caused by the cells of the Gastric mucosa descends. The causes of stomach cancer are among others Nitrosamines from food, nicotine and Helicobacter pylori discussed. In most cases, the tumor causes symptoms late, when it is already well advanced. Due to the late diagnosis, stomach cancer is often treated late, so that this type of cancer has a very poor prognosis for the patient.

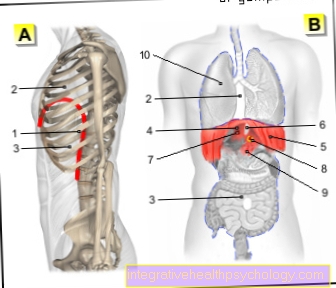
Stomach cancer
Gastric cancer
- Tumor (stomach cancer)
- Esophagus - Esophagus
- Stomach body -
Corpus gastricum - Duodenum -
Duodenum - Mucous membrane -
Tunica mucosa - Submucosal membrane -
Tela submucosa - Muscle wall -
Tunica muscularis - Serosa layer -
Tunica serosa
5 year survival rate:
Tumor stage I (90-100%)
Tumor stage II (80-100%)
Tumor stage III (10%)
Stage IV tumor (5%)
Important: gastroscopy
You can find an overview of all Dr-Gumpert images at: medical illustrations

frequency
The incidence peak of gastric cancer is beyond the age of 50, with men twice as likely to develop gastric cancer than women. The incidence of gastric cancer is falling worldwide. However, it is still the fourth most common tumor in men and the fifth most common in women. There is also an increased tendency in favor of carcinoma in the cardia area (= stomach entrance, see also anatomy stomach).
The disease rate is around 10 out of 100,000 people in Germany. In other countries, e.g. in Japan, gastric cancer is twice as common. It is believed that this is due to different eating habits, since the incidence rate is no longer higher among Japanese people who have emigrated to the United States and who have adopted American eating habits.
Read about the best nourishment in case of illness: Diet in cancer
Anatomy stomach

- Esophagus (gullet)
- Cardia
- Body
- small curvature
- Fundus
- great curvature
- Duodenum (duodenum)
- Pylorus
- Antrum
Symptoms and signs
Stomach cancer is usually a so-called "silent" tumor - that is, it does not make itself felt at all in the early stages or with only very unspecific symptoms. This often means that the cancer can grow over time and many of the first signs are blamed on a sensitive stomach or stress. The symptoms of gastric cancer only appear at an advanced stage and are usually very unspecific.
Almost all cancer diseases have characteristic symptoms - the so-called B symptoms. This includes recurring fever - often with only marginally elevated temperatures - unwanted weight loss in a short time and the appearance of night sweats. Other general tumor symptoms are poor concentration, fatigue, decreased performance and tiredness.
Many stomach cancer patients also report complaints in the gastrointestinal system. Pain in the upper abdomen can occur especially after or during the meal, often accompanied by heartburn, nausea, bad breath from the stomach and upper abdominal pressure. Vomiting can occur especially if the tumor is located at the entrance to the stomach (cardia) or the stomach exit (pylorus).
There are also frequent complaints about loss of appetite and reports of an unpleasant feeling of fullness even after small meals, often accompanied by a distended stomach and gas. It is precisely these signs that often occur in the context of other harmless diseases of the gastrointestinal tract or under severe stress and are therefore often not associated with serious cancer.
Therefore, it is important to consult your family doctor even if you have recurring heartburn or frequent severe flatulence so that he can diagnose the cause and treat it appropriately.
Another sign of stomach cancer is decreased appetite. Patients often feel a sudden aversion to certain foods - mostly meat - and suddenly no longer tolerate other foods. This phenomenon can also occur in other stomach diseases and other types of cancer (e.g. colon cancer).
In the late stages of the disease, gastric bleeding can occur, which is noticeable either by vomiting blood or black stools.
Read more about: Blood in the stool - these are the causes!
As the disease progresses, difficulty swallowing (dysphagia), especially with tumors in the area of the stomach entrance, and upper abdominal pain, increase.
As with almost every tumor disease, weight loss (tumor cachexia), increased body temperature (tumor fever) and reduced performance occur in the later stage. If cancer has spread (metastasis) in the abdomen, there may be an accumulation of fluid (ascites) and swelling of the abdomen. In rare cases, the tumor can even be felt in the abdomen.
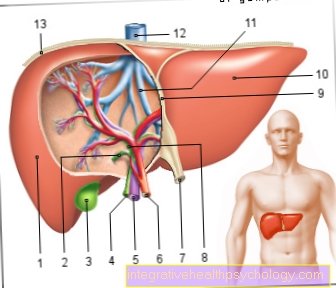
Existing daughter tumors in the liver (liver metastases) can lead to swelling and loss of function of the liver with yellowing of the skin (jaundice). If metastases (daughter tumors) occur in the skeleton, bone pain can occur, which is particularly severe and devastating.
If a large amount of bone tissue is destroyed by the tumor, pathological fractures can occur without an accident (e.g. vertebral body fracture, femoral neck fracture, etc.). Metastases in the lungs sometimes cause shortness of breath (dyspnoea) and coughing up blood (hematemesis).
Since stomach cancer is easy to treat, especially in the early stages, you should listen to your own body and not be afraid to see a doctor, even if you have general non-specific symptoms.
causes
The causes of gastric cancer are very diverse and the mechanisms by which it develops are still largely not understood. The risk of developing gastric cancer increases by a factor of 4-5 if the gastric mucosa is infected with the bacterium Helicobacter pylori. Half of all gastric cancer patients are also colonized with this bacterium. However, the bacterium is widespread and by far not all infected people will develop gastric cancer in the course of their lives.
They are also found in food carcinogenic (carcinogenic) pollutants often discussed as the cause. For example Nitrosamines, which occur, for example, in smoked, cured, grilled or seared meat products. Another pollutant is that Aflatoxinwhich are formed by certain molds in food and which also contain tumors in the esophagus and liver cause.
The Smoke of cigarettes and the consumption of hard liquor alcohol are also considered a risk factor for gastric cancer development.
The lack of certain vitamins can be assumed to be a contributing factor in the risk of cancer. As important Vitamins will be the Vitamins A, C, E described.
A certain one genetic risk is also important. People whose first-degree family members (e.g. parents) suffer from stomach cancer have an approximately 3 to 4-fold increased risk of developing a stomach tumor.
The has a special meaning Blood group A, as the carriers of this blood group tend to develop stomach tumors more often.
There are a number of Stomach disorders who are prone to developing gastric cancer.
The atrophic autoimmune gastritis (type A - gastritis) or that Menetrier syndrome (Giant gastritis), both chronic inflammations of the gastric mucous membrane, significantly increase the risk of developing stomach cancer.
Gastric polyps (Gastric mucosal growths), which are benign at first, can degenerate and become malignant over time. This process can be recorded in 20% of cases of gastric polyps, so that the removal of polyps in good time is recommended.
The connection between the Gastric ulcer (Gastric ulcer) and gastric cancer / gastric cancer is still unclear.
Although 5-10% of the misdiagnosed ulcers turn out to be gastric carcinomas, in retrospect you never know whether it was a gastric ulcer that has degenerated or whether the tumor just mimics the appearance of a gastric ulcer.
However, the fact is that a duodenal ulcer (ulcus duodeni) almost never degenerates.
Part of the stomach can be removed from the junction between the remaining stomach and the upturned stomach, even after many years Intestines Develop a carcinoma (anostomosis), so that check-ups with a gastroscopy must be done regularly.
This tumor is then also called "anostomy carcinoma".
Is Stomach Cancer Hereditary?
The cause of stomach cancer is mainly due to risk factors such as smoking or frequent stomach ulcers. Only in a few cases the stomach cancer is due to an increased familial risk.
However, it is said that the likelihood of developing stomach cancer if a first-degree family member has the disease is about 2-3 times higher. However, it is often not only genetic predisposition that is responsible for this, but also family risk factors such as the eating behavior.
As a rule, however, relatives are not given any additional check-ups such as Gastroscopy advised. However, if several family members have stomach cancer or if the cancer occurred at a young age, genetic counseling or increased check-ups can be considered.
diagnosis
The outcome of every diagnosis is the patient interview (Anamnese). You have to look for the above symptoms in particular and ask about frequent gastric cancers in the family. The existing risk factors such as nicotine and alcohol consumption should always be inquired about.
During the physical examination, in rare cases the tumor can be felt in the abdomen. Occasionally the Virchow's gland (lymph node) in the clavicle can be felt.
When analyzing the blood (Laboratory values) certain blood values can indicate a tumor disease. For example, a lower Blood pigment content (hemoglobin) in the blood indicate chronic blood loss due to tumorous bleeding. With the Hemoccult test a search is made for blood in the stool, which can occur in the case of chronic blood loss in the Gastrointestinal tract occur. So-called Tumor markers are substances in the blood that are often found in some types of cancer and can therefore indicate a cancer.
They do not play an essential role in the initial diagnosis of gastric cancer, as there are no reliable tumor markers for this disease. However, if a certain tumor marker value is found to be elevated before the operation, which disappears after the operation, this marker can be used as a control marker to prevent a new outbreak of the tumor (Tumor recurrence) Quickly diagnose with a blood test.
In order to be able to make a diagnosis of gastric cancer, a Gastroscopy be performed.
Illustration stomach cancer

- Stomach cancer
- great curvature
- Duodenum (duodenum)
- small curvature
- esophagus
Gastroscopy

The "mirroring" (Endoscopy) of the stomach is the method of choice for the direct assessment and classification of mucosal damage and should be carried out as soon as possible if a stomach tumor is suspected.During this examination, images from the tube camera (endoscope) that the patient must "swallow" are taken esophagus and transferred to the stomach on a monitor. During the endoscopy, tissue samples (biopsy) from suspicious mucosal areas and ulcers. Several samples (5-10) must be taken from a suspect area in order not to miss any malignant (malignant) tissue changes.
The tissue assessment under the Microscope (histological findings) is far more meaningful than the (macroscopic) findings recorded with the naked eye.
Only in the fine tissue (histological examination) can the suspicion of a tumor be proven and the Tumor type to be determined. The spread of the tumor into the layers of the stomach wall can also be determined.
X-ray swallow
During this non-invasive, imaging examination, the esophagus is x-rayed while the patient swallows an x-ray contrast medium. The contrast medium is deposited on the stomach and intestinal walls, whereupon they are accessible for an assessment.
The typical finding in gastric cancer is a tumor lump that protrudes into the inside of the stomach. However, it is also not uncommon to see a picture similar to that of an ulcer (stomach ulcer), so that no clear diagnosis can be made. This examination can also be used to assess the degree of constriction (stenosis) caused by a tumor.
Compared to gastroscopy, the assessment of changes in the mucous membrane is limited. In particular, the assessment between benign (benign) and malignant (malignant) changes is not possible. This requires direct assessment of the inside of the stomach by mirroring with tissue sampling (PE).
Tumor staging
- Determination of the tumor stage (tumor staging):
Once the diagnosis of gastric cancer has been confirmed, the stage of the tumor is then determined in order to plan further therapeutic approaches. Various methods are used to assess tumor spread, lymph node involvement and possible distant metastases.
- X-ray - chest (X-ray of the chest):
An overview x-ray of the chest (chest x-ray) can provide information about the involvement of the lungs and the affected lymph nodes in the middle layer (mediastinal).
Read more on the topic: Chest x-ray (chest x-ray)
- Ultrasound (endosonography (endoluminal ultrasound)):
With an endoscopic ultrasound, the patient first has to "swallow" a tube during a light anesthesia, as with a gastroscopy.
However, in this examination, an ultrasound head is attached to the end of the hose instead of the camera. With this method, the spread of the tumor in depth (infiltration), i.e. into the stomach wall, can be made visible by placing the transducer on the tumor and (regional) lymph nodes located in the epigastric region can also be assessed. - Computed Tomography (CT):
The spiral computed tomography (spiral CT) can provide information about the extent of the tumor, the spatial relationship to neighboring organs, the lymph node involvement and also about distant metastases. You need a CT of both the chest (thorax) and the abdomen (abdomen) in order to be able to assess all metastatic routes. Magnetic resonance imaging (MRI) also provides similar results. In the course of the disease, a CT or MRI of the skull may be necessary to diagnose brain metastases.
Read more on the topic: Computed Tomography
- Sonography:
With sonography (ultrasound) the abdominal organs are assessed non-invasively and without exposure to radiation. With the ultrasound of the abdomen (abdomen), for example, metastases in the liver or affected lymph nodes can be revealed. Since the method is easy to use and does not burden the patient, it can be repeated many times without hesitation and used for follow-up and follow-up care.
- Skeletal scintigraphy:
Skeletal scintigraphy is a nuclear medical imaging examination and is used as part of tumor staging to detect distant metastases in the skeleton. For this purpose, the patient is given a radioactive substance intravenously and then the distribution of the radioactive substance in the bone is made visible with a special camera (gamma camera). The radioactive substances accumulate in the bones and are found in increased numbers where bone remodeling and repair processes are in progress. In the area of the bone metastases, for example, an increased accumulation of the radioactive substance can be seen.
- Laparoscopy (laparoscopy):
In advanced tumor stages, it is sometimes necessary to perform a laparoscopy in order to correctly assess the regional extent and any involvement of the peritoneum (peritoneum cancer) and the liver (metastases). During this procedure, which is carried out under general anesthesia, various instruments and a camera can be inserted through small incisions in the abdominal skin and the tumor spread can be observed directly.
Is Stomach Cancer Curable?
Whether gastric cancer is curable depends on various factors. The decisive factor here is above all Time of diagnosis - The earlier gastric cancer is diagnosed, the better the chance of recovery.
The so-called 5-year survival rate in stage 1 (here the tumor has not yet affected any daughter tumors or lymph nodes) is over 90%. In the final stage 4 it is only just under 5%.
This is because in the treatment of gastric cancer, removal of the affected area of the stomach is the method of choice - possibly with a previous one chemotherapy. If the tumor can be completely captured and removed, the chances of recovery are very good. However, if tumor tissue persists, the cancer can enlarge again.
If an operation is not possible or daughter tumors have already formed in other organs, it must be assumed that, as a rule, the cancer will not be permanently cured. However, there is the possibility of keeping the tumor “in check” for a longer period of time and thus extending the patient's life.
A relapse with renewed tumor formation years later (so-called recurrence) is also possible. The chances of recovery depend on the type of tumor and the time of diagnosis.
course
The course of cancer is divided into different stages. The decisive factor here is how spread the tumor is and whether it has affected lymph nodes or other organs.
If the stomach cancer is in the early stages, it is relatively small and can only be found in the superficial layers of the gastric mucosa. If the tumor now begins to grow, it spreads in the stomach and also penetrates into the deeper tissue layers of the gastric mucosa.
Finally, it can happen that he also ins Peritoneum or penetrates the surrounding lymph nodes and reaches other organs, for example via the bloodstream - this is called distant metastases (daughter tumors).
In stages I-III there are no distant metastases and only isolated lymph node involvement. The final stage IV is present as soon as a daughter tumor is present.
The course of the disease varies from patient to patient and depends to a large extent on how early the therapy is started and how well it works. If there are daughter tumors, these trigger different complications depending on the organ affected. Therefore, every affected patient should speak directly to the doctor treating them about the likely course of their illness.
End-stage gastric cancer
Unfortunately, it is not yet possible to cure every form of stomach cancer today. If one speaks of the terminal stage, one means that the cancer cannot be fought completely. This can have several causes.
The stomach cancer is common recognized too late and has already formed so-called metastases - that is, tumor cells have settled and are now forming daughter tumors in other organs. Some tumors can also inoperable because they are too close to large blood vessels - or even grown together with them - and such a removal is no longer possible.
Also, some patients are no longer in one physical conditionwho allow an operation, for example because they suffer from severe comorbidities or because their old age makes an operation too dangerous.
If a patient is in such an end-stage gastric cancer, the therapy no longer focuses on defeating the cancer once and for all, but rather on enabling the person affected to live as long and pain-free as possible. This approach is sometimes referred to as Palliative therapy.
Palliative therapy consists of several pillars. On the one hand, one tries to limit the cancer growth and thus the affected person as much time as possible to give, on the other hand one tries to occur To alleviate accompanying complaints as best as possible. The latter often mainly includes individual pain therapy, as stomach cancer, but also its possible daughter tumors, can cause severe pain.
Concomitant symptoms such as heartburn and overinflation are also reduced. Complications such as the formation of Ascites or an acute one Gastric bleeding these can also be treated - often as an inpatient.
In the further course, patients also need help with food intake. For example, the tumor can form a constriction in the stomach that food can no longer get past. There are also several treatment options for this, which must be discussed and decided in close cooperation between doctor, patient and relatives so that the patient can live with it in the long term. Training for relatives and patients or the commissioning of a nursing service are often necessary.
In order to keep the tumor small for as long as possible, there are various options that can be discussed and selected individually with the attending physician. The type of stomach cancer plays a decisive role in whether a therapy option can work.
So can a chemotherapy or Irradiation be helpful. For a few tumors, there are now also drugs that work with specific antibodies and can thus "attack" the tumor directly.
Finally, one should not ignore the emotional burden caused by the disease. Hospitals often offer too psychological help and a social service that can help patients and relatives with further organization of care and related problems. Such a place can also be organized in a palliative medical ward, in which the patient can be given the most pleasant possible last time with the help of specialists.