meniscus
Synonyms in a broader sense

Cartilage disc, anterior horn, pars intermedia, posterior horn, inner meniscus, outer meniscus,
English: meniscus
definition
The meniscus is a cartilaginous structure in the knee joint that helps transfer force from the thigh bone (femur) to the lower leg bone (shin / tibia).
The meniscus aligns the round thigh bone (femoral condyle) with the straight lower leg (tibial plateau).
Damage to the meniscus, such as meniscus tears, leads to increased stress on the cartilage. The consequence is premature wear of the knee joint cartilage. As a result, osteoarthritis of the knee can develop.
Therefore, the meniscus plays an important role in our knee joint.
Appointment with a knee specialist?

I would be happy to advise you!
Who am I?
My name is I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
But now enough is indicated ;-)
The knee joint is one of the joints with the greatest stress.
Therefore, the treatment of the knee joint (e.g. meniscus tear, cartilage damage, cruciate ligament damage, runner's knee, etc.) requires a lot of experience.
I treat a wide variety of knee diseases in a conservative way.
The aim of any treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- - your orthopedic surgeon
14
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
Further information about myself can be found at
anatomy
The meniscus is found in the knee joint. Per Knee joint one can find one Medial meniscus and one External meniscus.
Of the meniscus lies on the side of the knee joint between the upper and lower leg.
It consists of elastic fiber cartilage that can adapt to the movements of the knee joint.
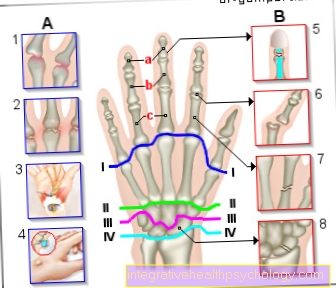
Figure meniscus

- Inner meniscus -
Meniscus medialis - Inner articular knot
(Shinb.) -
Medial condyle - Transverse ligament of the knee joint -
Lig. Transversum genus - Kneecap ligament -
Ligamentum patellae - Bursa - Bursa
- Outer meniscus -
Lateral meniscus - Outer joint nodules
(Shinb.) -
Lateral condyle - Anterior cruciate ligament -
Lig. Cruciatum anterius - Posterior cruciate ligament -
Ligamentum cruciatum posterius - Femur - Femur
- Shin - Tibia
- Kneecap - patella
You can find an overview of all Dr-Gumpert images at: medical illustrations

Meniscus parts
The meniscus is divided into 3 parts:
- Anterior meniscus
- Pars intremedia
- Meniscal posterior horn
The medial meniscus posterior horn is most commonly affected in the case of medial meniscus damage.
Medial meniscus
The inner meniscus, together with the outer meniscus, is part of the Knee joint. It is a C-shaped fiber cartilage that extends between the two articular surfaces of the Thighbone and des Shin are located. The meniscus enlarges the joint surface and ensures even pressure distribution. The menisci serve as "shock absorbers" and stabilize the joint.
The medial (inner) side of the medial meniscus is fixed to the Joint capsule and the inner collateral ligament (Inner band) grown together and therefore not very movable. Because of this anatomy, the inner meniscus is more often affected than the outer meniscus in sports injuries. In normal movement, the medial meniscus is at the External rotation under tension and is less stressed during internal rotation.
Different sports such as tennis, handball, soccer or skiing can put a lot of stress on the meniscus. But also with increasing age the meniscus loses thickness and it comes to wear. Even normal movements or just a little force can be enough to tear the meniscus and cause pain. An injury to the medial meniscus can also be combined with a Cruciate ligament tear and one Inner ligament tear occur together, this combination of injuries is also known as "Unhappy triad“.
Depending on the occurrence of the meniscus injury, the symptoms are different. Is it a traumatic Injury, such as can occur in a twisting-falling movement, is felt by the person concerned suddenly Pain in the joint space when walking or turning. In the event of an injury, part of the meniscus can also be pinched and the affected person has limited ability to stretch and bend the knee joint.
Is the injury a Wear and tear, which is caused by degeneration, the Smpytoma are more general. The affected person feels increasing stress pain in the knee joint and possibly additional instability.
Diagnosis is based on both anamnesis and different ones Meniscus mark approach. Checking the pain during internal and external rotation, palpation (palpation) of the knee joint, and the mobility of the knee joint can help in the diagnosis. Also be MRI of the knee - and X-rays prompted to also assess the bony structures.
Therapeutically, attempts are made to sew up mensic tears, especially in young patients, and to preserve the cartilage. Depending on the prognosis, certain sports activities should be avoided in the event of severe injuries; this should be discussed in detail with the doctor. In addition, there is a risk of earlier osteoarthritis of the knee joint in contrast to uninjured knees.
External meniscus
The outer meniscus is a sickle-shaped element in the knee joint made of fiber cartilage, which is also between the articular surfaces of the femur and shin. Like the inner meniscus, the outer meniscus also has the task of To cushion shocks and to distribute the loading pressure evenly over a larger area.
In contrast to the inner meniscus is the outer meniscus Not grow together with the joint capsule and the outer collateral ligament (outer ligament), which is why the outer meniscus is less affected by injuries than the inner meniscus. The opposite of the inner meniscus is the outer meniscus in the Internal rotation loaded and relieved during external rotation. It also acts as a slide bearing between the joint surfaces and helps, among other things, to better distribute the synovial fluid in the knee joint and thus to ensure better sliding ability.
If an injury does occur on the outer meniscus, this can be traumatic as well as due to wear and tear, as with the inner meniscus. The assessment of the injury is also similar to that of the medial meniscus damage. Clinical Meniscus mark and imaging tests help diagnose. The therapeutic approach and the prognosis of the medial meniscus lesion are also the same (see above).
Functions of the meniscus
The individual tasks should, however, be presented again in brief here.
The menisci in the area of the knee joint have the following tasks or functions:
- The increase in the contact area
- Stabilization
- Buffer or shock absorber function
Enlargement of the contact area:
The knee joint connects the thigh (= femur) with the lower leg (= tibia). Since both legs have a different structure and thus also a different joint surface, they would only form a small contact surface if they were placed on top of one another without a knee joint and menisci. In order to avoid this instability and dysfunctionality, the menisci arose in the course of human development, which - from a technical point of view - could also be referred to as "washers".
Stabilizer:
Stabilizing functions are particularly attributed to the posterior horn of the meniscus. It sits like a brake pad between the tibia and femur and prevents the tibial head from sliding forward.
Buffer function:
Due to the great elasticity that results from the fibrous structure of the cartilage tissue of the menisci, impacts from the thigh to the lower leg are buffered. A comparison with shock absorbers in a car is appropriate here.
function
The function of the meniscus is to act as a shock absorber to transfer the force from the thigh to the lower leg (shinbone = tibia). Due to its wedge-shaped appearance, the meniscus fills the gap between the round thigh roller (femoral condyle) and the almost straight tibial plateau (tibial plateau).
When moving, the elastic meniscus adjusts.
It also has a stabilizing function as a “page limiter”.
The synovial fluid is better distributed through the meniscus.

Blood flow to the meniscus
The meniscus is very poorly supplied with blood!
- Red zone: close to the capsule = good blood circulation
- Red and white zone: limited blood flow
- White zone: no blood flow
Diseases
The most common disease of the meniscus is the meniscus tear / Meniscus damage. Since the meniscus is only supplied with blood in its peripheral zones, it has only a limited potential for regeneration. In old age, meniscus wear (meniscus degeneration) is normal.
Further information on the treatment of damaged menisci can be found here:
- Meniscus treatment
Meniscal tear
Injuries to the meniscus are among the most common knee injuries and are not uncommon Result of a sports accident.
Typical injury mechanism can e.g. a unfortunate fall on ski vacation be: Affected people lose control on the slopes, a ski gets stuck in the deep snow during that Knee joint is twisted by the force of the fall. Act like that massive shear forces on the meniscus including overstretching and tearing!
Older patients can also use one wear-related (degenerativeSuffer a meniscus tear without previous trauma.
Is preferred inner meniscus concerned as he was with the Inner knee ligament is firmly grown and therefore has fewer opportunities to evade rotary movements.
More common than isolated meniscus damage are combined ligament injuries. For example anterior cruciate ligament, Inner knee ligament and Medial meniscus tear at the same time! One then speaks of a "Unhappy triad“.
Characteristically, an acute meniscus tear is characterized by three symptoms ("Symptom triad") accompanies:
1.) pain
Patients report severe, immediately shooting pain in the affected knee joint. Both strain and pressure are very painful.
2.) Blocking
By e.g. Entrapment of the torn meniscus ends can do that Knee joint mechanically block.
Affected people describe a kind of "Snap“Over the joint.
It creates a Knee stiffnessespecially when attempting to stretch.
3.) swelling
If the base of the meniscus is well supplied with blood, it develops within a few minutes extensive hematoma ("bruise") accompanied by a severe swelling.
The next day at the latest is also a Joint effusion to observe.
In order to secure the diagnosis of a meniscus tear, the attending physician conducts targeted Pain provocation and pain tests by.
This includes e.g. the Steinmann I sign: The patient bends his knee at a 90 degree angle while the examiner jerks the knee outwards. If pain occurs in the area of the internal joint space, this is an indication of a Medial meniscus injury to evaluate.
In addition to manual examinations, an urgent suspicion is essential imaging procedure be applied.
In principle, are suitable for this X-rays, however, fresh injuries cannot be seen in the vast majority of cases.
Nowadays, therefore, that becomes MRI (Magnetic resonance tomography) is used as the gold standard for confirming diagnoses.
Without radiation exposure, high-resolution images can provide clarity.
Depending on the question, the Administration of contrast media to be required.
Experienced investigators can even repair the injury with a suitable one Ultrasound machine represent.
Therapeutically, in very rare cases, in addition to surgical therapy, a conservative (non-surgical) option is available. This includes treatment with anti-inflammatory tablets and ointments, injections of local anesthetics or physiotherapy.
Meniscus OP (arthroscopy)

Nowadays the standard therapy for meniscal tear is the arthroscopic treatment.
By minimally invasive technique ("Keyhole principle") a tiny camera and surgical instruments are integrated into the Knee joint introduced.
Advantages are one lower complication rate, shorter healing phase, as well as clearly minor surgical scars (about 5-10 mm).
Open meniscus surgery are only used in individual cases and in the event of severe accompanying damage, e.g. Broken bones or massive further ligament injuries, carried out.
If possible, the meniscus should always be preserved! Nevertheless, the method used is always based on Injury severity, possible Accompanying damage and individual overall constitution.
In the best case, the torn ends can simply be sewn again (Meniscal Refixation). This method is aimed particularly at young and active patients without any cartilage changes caused by wear.
However, there is no real upper age limit.
Great advantage, the possible full function recovery of the knee joint.
In the ideal case, those affected can regain their complete, athletic performance!
In individual cases, however, the longer rehabilitation phase required to be viewed as.
Because with the meniscus refixation, something has to be done six-month sports break be respected. This also applies to knee-stressing activities in the context of professional life, e.g. Tiling or gardening.
Therefore, some patients choose one, despite theoretically possible refixation partial removal of the meniscus (Partial meniscal resection).
During this procedure, the doctor removes the damaged, unrecoverable meniscal tissue. This is usually followed by a Joint irrigationso that any remaining fragments can also be removed.
In the foreground is a desired one Symptom-, in particular Freedom from pain.
Despite the most modern arthroscopic technology, not every meniscus can be preserved.
The total distance (Meniscusectomy) but carries many risks, such as Osteoarthritis of the knee, and should be used very cautiously.
Therefore, in recent years, there have been an increasing number of methods for Meniscus transplant developed.
However, the long-term successes are not yet 100% assured, so it remains to be seen which possibilities will open up.
The most common complication of the Arthroscopy is a violation of Saphenous nerve. It is a purely sensitive nerve and supplies the skin on the inside of the lower leg.
Due to pressure damage or a knot during arthroscopy, patients feel Paresthesia (Tingling, numbness etc.) in the affected area.
However, in most cases these symptoms disappear after a few months without any external intervention!
Unfortunately, the "Rerupture rate“, So the rate of renewed meniscus tear after the operation, at about 25%!
Particularly affected are patients in whom a recovery of the anterior cruciate ligament is done.
Another long-term consequence is the increased tendency to develop Osteoarthritis of the knee, i.e. age-related wear of the cartilage surface.
Basically, the more meniscus had to be removed, the higher the risk of developing osteoarthritis.
But why is that so? Our menisci have a kind of "Shock absorber effect“Within the knee joint. If they are missing or only partially present, the weight and load will be distributed unevenly in the joint.
As a result will be remaining cartilage components overused- there is one arthrosis.
After the arthroscopy, the follow-up treatment takes place. Depending on the extent of the intervention, the knee joint must either be immobilized for some time (e.g. using crutches) or physiotherapy can be started right away.