Non-Hodgkin lymphoma
Definition - What is Non-Hodgkin Lymphoma
Non-Hodgkin lymphomas are a large group of different malignant diseases that have in common that they originate from lymphocytes. The lymphocytes belong to the white blood cells, which are essential for the immune system. Colloquially, the non-Hodgkin lymphoma and the Hodgkin lymphoma are summarized under the lymph node cancer. The division into these two groups is historical, but is still used today. The various non-Hodgkin lymphomas differ in their malignancy and in the cell of origin.
Read more on the topic: Lymph node cancer

causes
There are a few known factors that can favor certain non-Hodgkin lymphomas. First of all, cell damage should be mentioned here. This can be triggered by previous radiation treatments or chemotherapy treatments for previous cancers. Since these therapies do not only have their effect on the tumor, healthy body cells are also damaged, which can result in non-Hodgkin lymphoma.
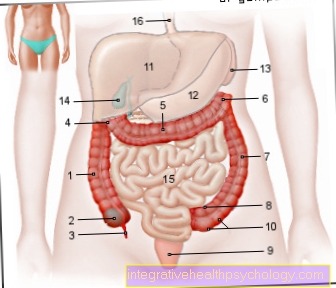
Furthermore, excessive contact with benzenes, which were previously used as solvents, can lead to cell damage. In addition to these global causes, there are also causes that increase the risk of specific subtypes of non-Hodgkin lymphoma. For example, an infection with the Ebstein-Barr virus, which causes Pfeiffer glandular fever, or an HIV infection can promote Burkitt's lymphoma. Burkitt's lymphoma is considered to be very aggressive and originates from the so-called B lymphocytes. Infections with bacteria, such as the bacterium Helicobacter pylori, can also promote a certain non-Hodgkin lymphoma. The infection triggers an inflammation of the stomach (gastritis) and later on it can develop into MALT lymphoma (Mucosa Associated Lymphoid Tissue).
Read more about our main article: Lymphoma
Concomitant symptoms
The classic symptom of non-Hodgkin lymphoma is a lymph node that is swollen over a long period of time and does not hurt. These can often be felt on the neck, in the armpit or in the groin. The B symptoms, which are a combination of the three symptoms fever, weight loss and night sweats, are also typical. In advanced stages, the spleen can enlarge so that it can be felt under the left costal arch. This enlargement can be painful. Another late symptom is the decrease in all blood cells. This is triggered by the fact that the bone marrow is damaged as the disease progresses and thus the production of blood cells is restricted. This then manifests itself with a number of symptoms, such as fatigue and weakness, as well as spontaneous bleeding. These can manifest as nosebleeds or bleeding gums. In addition, there is a tendency to frequent infections, as the body's defense cells are reduced and partially changed and therefore functionless. In rare cases, masses can occur in the ear, nose and throat area, in the entire digestive tract or on the skin.
Read more in our main article: Symptoms of lymphoma
What are the symptoms on the skin?
Changes to the skin do not appear in all non-Hodgkin lymphomas and, depending on the subtype of non-Hodgkin lymphoma, different symptoms appear on the skin. Chronic lymphocytic leukemia, for example, can be accompanied by itching and chronic hives. The hives show up on the skin with redness and small localized swellings. In addition, large areas of the skin can become red (erythroderma) and skin fungi can occur. These symptoms appear on the skin, especially in elderly patients. In T-cell lymphomas, mycosis fungoides and Sézary syndrome in particular cause symptoms on the skin. With mycosis fungoides, reddened areas with scaling and pronounced itching appear first. These slowly develop into so-called plaques. Thickening of the skin is typical. In the late stages, hemispherical skin tumors can be found that show open areas on the surface. The mycosis fungoides can turn into a Sézary syndrome, which progresses with extensive redness, severe itching and excessive cornification of the hands and feet.
B symptoms
The B symptoms describe a complex of three symptoms: fever, weight loss and night sweats. The definition of fever is not always consistent in the specialist literature. As a rule, one speaks of a fever at body temperatures that are over 38 degrees Celsius. The fever must not be explainable by another illness, such as an infection.
A weight loss of more than 10% of the original body weight within six months is also part of the B symptoms. The third symptom is night sweats. Night sweat describes waking up bathed in sweat in the middle of the night. Patients often report that they have to change their pajamas or bedding several times a night. The term was coined by the Ann Arbor classification. With the addition of "A", the symptoms mentioned are not present. If the suffix “B” is used, the symptom triad is present in the patient. In most cases, the presence of B symptoms is associated with a poorer prognosis, as they are an expression of high disease activity of the tumor. They usually decrease after therapy has been initiated. If this is not the case, the therapy must be reconsidered and, if necessary, changed, as persistent B symptoms tend to suggest a non-response to chemotherapy.
Find out more about this topic at: B Symptoms
What is the life expectancy with non-Hodgkin lymphoma?
The life expectancy of the individual non-Hodgkin lymphomas is very different, which is why no general statement can be made. On the one hand, it depends on how malignant and how advanced the non-Hodgkin lymphoma is at the time the diagnosis is made. The following are the life expectancies for some common non-Hodgkin lymphomas.
- Follicular lymphoma has a life expectancy of approximately 10 years at the time of diagnosis.
- Life expectancy with mantle cell lymphoma is lower at around 5 years.
- In multiple myeloma, many factors play a role in the calculation of life expectancy, so that it is difficult to make a statement here. In the best case, in young patients with optimal therapy, about 50% of the patients survive the next 10 years.
- Burkitt's lymphoma can lead to death within months if diagnosed late, whereas early detection with directly connected therapy shows a good life expectancy. However, this good prognosis is worsened as soon as a second tumor occurs, which is not atypical in Burkitt's lymphoma.
- Mycosis fungoides is one of the less malignant lymphomas and therefore life expectancy in its early stages is good. However, if invasive growth occurs in other organs, life expectancy deteriorates significantly.
You can find detailed information at: The prognosis for a lymphoma
What are the chances of recovery?
When considering the chances of recovery, one has to consider the malignancy of non-Hodgkin lymphoma. In the case of the less malignant lymphomas, a cure can only be assumed in the early stages. The slow growth makes the therapy very difficult, so that only the small findings can be completely cured with the radiation. In the higher stages there is no longer any chance of recovery and this is not the aim of therapy. The malignant non-Hodgkin lymphomas are curable to a very high percentage in the early stages. Even in advanced stages, a cure can be assumed in up to 60% of cases.
You may also be interested in this topic: The prognosis for a lymphoma
to form
Non-Hodgkin's lymphomas are divided into four groups. Depending on the cell of origin, they are divided into B-cell and T-cell lymphomas. In addition, a further distinction is made with regard to the malignancy (malignancy). The naming is often based on how the cells change malignantly in the specific lymphoma.
Forms of B-cell lymphomas
Less malignant B-cell non-Hodgkin lymphomas include:
- chronic lymphocytic leukemia
- Hairy cell leukemia,
- Waldenström's disease,
- Multiple myeloma,
- Follicular lymphoma,
- MALT lymphoma
- Mantle cell lymphoma.
Less malignant here means that the lymphomas show slower growth. However, treatment with chemotherapeutic agents is rather difficult because they work better when it comes to fast-growing tumors.
The more malignant B-cell lymphomas include:
- Burkitt lymphoma
- diffuse large-cell B-cell lymphoma
- anaplastic lymphoma
Burkitt's lymphoma is often associated with an infection with the HI virus. The more malignant lymphomas show faster and invasive growth. Because of the high rate of cell division, they respond well to chemotherapy.
Forms of T cell lymphomas
There are also many subtypes of T-cell lymphomas that are classed as less malignant lymphomas:
- Mycosis fungoides
- T-zone lymphoma
- NK cell leukemia (natural killer cell leukemia),
- angioimmunoblastic T-cell lymphoma
- pleomorphic small cell lymphoma.
In the case of malignant T-cell lymphomas, a distinction is made between anaplastic, lymphoblastic and immunoblastic lymphoma.
B-cell non-Hodgkin lymphoma
B-cell non-Hodgkin lymphoma is the most common non-Hodgkin lymphoma at 30%. It is one of the more vicious and aggressive forms. As with the other non-Hodgkin lymphomas, the diagnosis is made from a combination of a doctor's consultation with a clinical examination of the lymph nodes, as well as laboratory values and a lymph node biopsy (tissue sampling).Imaging is also done in some cases.
Read more on the subject at: Lymph node biopsy
In contrast to other non-Hodgkin lymphomas, there is no special marker in B-cell non-Hodgkin lymphoma that can be determined in the blood, for example, in order to be able to make a reliable diagnosis. Therefore, one is dependent on a biopsy of an altered lymph node. Since it is a malignant non-Hodgkin lymphoma, which is associated with rapid growth, therapy is almost always assumed to be cured. The healing rates are approximately 50% to 90%. The therapy consists of chemotherapy. Which chemotherapy is given depends on the age and on a certain degree of risk, which is calculated as part of the diagnosis. Usually, a combination of different chemotherapy drugs with a special antibody is given. In B-cell non-Hodgkin lymphoma, the 5-year survival rate is between 60% and 90%. Life expectancy depends on the genetic composition of the tumor and is worsened by factors such as old age, poor general condition and advanced stage according to the Ann-Arbor classification.
treatment
The choice of therapy is based on how malignant the non-Hodgkin lymphoma is. Less malignant lymphomas that are still in the early stages and that have not yet spread significantly are only irradiated, since chemotherapy is not sufficiently effective for slowly growing lymphomas. If the lymphoma is already further spread in the body, i.e. in stage III or IV according to Ann-Arbor, one can no longer assume that the disease will be cured. In this case, the patient is closely monitored and possible symptoms treated or a combination of different chemotherapeutic agents can be used.
The very malignant non-Hodgkin lymphomas are all treated with the aim of healing. The stage is not relevant either. The therapy of choice is a combination of several chemotherapy drugs. Studies have shown this to be more effective than using just a single chemotherapy drug. In addition to the general therapeutic approaches listed, there are specific treatment plans for certain subspecies of non-Hodgkin lymphoma, which are regularly updated according to the current study situation. This is the case, for example, with chronic lymphocytic leukemia or multiple myeloma.
Read more on the topic: Therapy of lymphoma
chemotherapy
Chemotherapy aims to interrupt the division process of the malignant cells of non-Hodgkin lymphoma. The various chemotherapeutic agents target different parts of the DNA in order to cause damage to it. As a result, the cell goes under and is broken down. The chemotherapy does not only act on the degenerated cells but also on the healthy cells of the body. The mucous membrane cells of the gastrointestinal tract and the bone marrow are particularly affected. The death of these cells can be used to derive the side effects of chemotherapy, which can include diarrhea, fatigue, a tendency to infection and spontaneous bleeding. For many of the non-Hodgkin lymphomas, so-called polychemotherapy according to the CHOP scheme is used. It is a combination of the following chemotherapy drugs: cyclophosphamide, doxorubicin, vincristine, and prednisolone. The former three drugs belong to the class of chemotherapy drugs. Prednisolone is a glucocorticoid, just like cortisone.
Here is the main article: chemotherapy
Stem cell therapy
Stem cell therapy can be considered if non-Hodgkin's lymphoma was not cured despite chemotherapy. A distinction is made between autologous and allogeneic bone marrow transplants. In autologous transplants, after very strong chemotherapy, which can kill all lymphoma cells, the patient is given their own bone marrow to replace the blood-producing system in the bone marrow. In the case of allogeneic transplantation, the patient receives bone marrow from a foreign donor that matches the patient in certain genetic markers.
You can read more about this under: Stem cell transplant
Irradiation
Radiation is used for the less malignant non-Hodgkin lymphomas. The affected lymph nodes are selected as the radiation field. If other tissues are also affected by invasive growth of the lymphoma from the lymph node, these can also be irradiated. The radiation therapists try to keep an important balance during radiation. On the one hand, the affected tissue should receive as much radiation dose as possible so that effective tumor control is possible. On the other hand, the surrounding tissue should be spared as much as possible. If the bones are brittle due to non-Hodgkin's lymphoma or if severe pain is felt there, the radiation can help to strengthen the bones again and to alleviate the pain.
You can find our main article at: radiotherapy
diagnosis
The diagnosis is made up of various methods. First, typical findings can be obtained through a conversation with the patient and a clinical examination, such as enlarged but not painful lymph nodes on the neck or in the groin region. B symptoms (the combination of fever, night sweats and weight loss) also suggest the presence of a malignant disease. In addition, a blood test is done and a suspicious lymph node is removed and then examined under the microscope. An imaging examination may be performed to complete the diagnosis.
What do the blood values show?
The normal blood count is used to check whether there is an increase or decrease in lymphocytes. Furthermore, it is checked whether the other blood cells show abnormalities, which can lead to anemia (anemia) with fatigue, for example. One reason for anemia is a breakdown of the red blood cells, which can also be detected in the blood count.
There are also specific values in the blood values that increase when there is inflammation. In this case, the inflammation parameters, such as CRP (C-reactive protein), would be increased. Specific blood tests may also be done to identify the exact subtype of non-Hodgkin lymphoma. For this purpose, certain surface proteins are determined using a biochemical method, which help to differentiate whether the non-Hodgkin lymphoma originates from the B lymphocytes or the T lymphocytes. These two groups are subgroups of lymphocytes that perform different tasks for the immune system.
What stages are there?
The stages are categorized according to the Ann-Arbor classification.
In stage I, only one lymph node region is affected or an infection outside the lymph nodes (extranodal infection), but within certain regions. A lymph node region refers to fixed groupings of lymph nodes, such as those found on the neck, in the armpit or in the groin. As an organ of the immune system, the spleen is also classified as a lymph node region. Extranodal infestation is when cells that are degenerate due to neighbors spread to other tissues.
In stage II, at least two lymph node regions or neighboring regions outside the lymph nodes are involved. However, these are all either above or below the diaphragm. This is a membrane made of muscles and tendons and separates the chest from the abdomen.
If the affected lymph nodes or the extranodal involvement are on both sides of the diaphragm, it is called stage III according to Ann-Arbor.
Stage IV is independent of the status of the lymph nodes and is awarded if at least one organ is affected and this cannot be explained by neighborhood relationships.
Metastases
By definition, a metastasis is the settlement of a malignant disease in a distant organ. The degenerate cells of non-Hodgkin lymphoma are usually initially located in the lymph nodes. However, they can also be distributed throughout the body with the bloodstream and settle in a different location. If this affects any organ of the body, one would assign stage IV according to the Ann Arbor classification.
What are the long-term effects?
With the various non-Hodgkin lymphomas there is a different risk of disease relapse. This is often more difficult to treat and should be discovered as early as possible with structured follow-up care. The use of multiple chemotherapy drugs increases the risk of developing a second tumor in the course of life. Typical of these secondary tumors are breast cancer, thyroid cancer or acute myeloid leukemia, a form of white blood cancer. Radiation can also trigger long-term effects. The organs that are in the vicinity of the irradiated lymph nodes are affected. Reddening and changes in tissue can be perceived on the skin. Inflammation can occur in the lungs, which can be associated with remodeling processes and possibly shortness of breath. Heart damage as well as nausea and fatigue are also possible.