Shoulder pain
Synonyms in a broader sense
- Shoulder pain
- Impingement Syndrome
- Tendinosis calcarea
- Rotator cuff tear
- Biceps tendon tendinitis
- AC joint osteoarthritis
- Osteoarthritis of the shoulder (omarthrosis)
- Supraspinatus tendon syndrome
introduction
The majority of people experience shoulder pain at some point in their life. These can be caused by an injury, but can also develop and progress slowly as part of certain diseases.
At acute Shoulder pain is a complaint that does not last longer than six weeks.
If the pain persists between six and twelve weeks, this pain is considered to be subacute.
Chronic After all, pain lasts longer than twelve weeks. Below are some of the causes that can lead to shoulder pain.

Pain in the neck, throat and upper arm
Acute attacks of pain in the neck and shoulder area are often caused by muscle tension. Possible triggers are drafts or cold, a cramped posture, incorrect sitting or lying down, and an unusually high level of stress. Mental problems can also lead to muscle tension.
Muscle strains are less common. This must be distinguished from recurring pain that radiates from the neck and neck into the shoulder. They often develop due to wear and tear in the cervical spine from too little or incorrect movement and a lot of sitting. The intervertebral discs become flatter, the cervical spine ossifies and the small vertebral joints wear out (facet joint arthrosis). This causes pain in the neck area and leads to an increasingly stiff neck. In addition, the muscles harden, which causes additional pain up to the shoulder. Acute pain attacks can then be triggered by drafts or cold. In addition, these processes pave the way for later nerve root compressions.
In the case of pain in the neck and shoulder that radiate into the arm, nerves are usually pinched immediately after they leave the spinal cord (Root compression). The nerve roots must pass through a narrow bony opening in the immediate vicinity of the respective intervertebral disc.
In most cases, especially in the elderly, the above wear-related processes are responsible for entrapment.
Slipped discs in the cervical spine, protruding discs in the cervical spine or whiplash injuries to the cervical spine (e.g. car accident) are less common. The consequences of root compression are sensory disturbances and pain in the neck, shoulder and in circumscribed areas on the arm. This can be accompanied by slight paralysis of certain muscles and possibly weakening of reflexes. Depending on the pinched nerve root, the symptoms appear in different places. The pain usually depends on the posture and is more severe at night.
Read more about this topic below: Shoulder Neck Pain - What You Should Know About It
Appointment with a shoulder specialist

I would be happy to advise you!
Who am I?
My name is Carmen Heinz. I am a specialist in orthopedics and trauma surgery in the specialist team of .
The shoulder joint is one of the most complicated joints in the human body.
The treatment of the shoulder (rotator cuff, impingement syndrome, calcified shoulder (tendinosis calcarea, biceps tendon, etc.) therefore requires a lot of experience.
I treat a wide variety of shoulder diseases in a conservative way.
The aim of any therapy is treatment with full recovery without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- - your orthopedic surgeon
14
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
You can find more information about myself at Carmen Heinz.
In the case of pain that radiates from the shoulder into the arm, there may be irritation of individual nerves. In most cases, this is due to carpal tunnel syndrome. A nerve (median nerve) is pinched at the wrist. Repetitive activities by hand, for example typing on a computer keyboard, encourage this. The pain usually occurs at night, radiates from the hand to the shoulder and is acutely improved by moving the arm. Sensory disturbances in the fingers can also occur as well as awkwardness of the fingers in the morning.
Furthermore, nerves in the nerve network between the cervical spine and shoulder, in the so-called cervicobrachial plexus, can be damaged. This can be caused by acute allergic-inflammatory processes (neuralgic shoulder amyotrophy). Substance abuse, infections, rheumatic diseases or overuse can all be triggers. The motion-independent pain usually begins suddenly, at night and on the dominant arm side. Hours later, they turn into muscle weakness of the shoulder muscles, which can appear in the long term in the form of a protruding shoulder blade and slowly recede. Sensory disturbances are more in the background.
Other reasons for damage to the nerve plexus are tumors or metastases, late damage caused by radiation, infections (e.g. Lyme disease) and certain sporting activities (hockey, shooting). Carrying a heavy rucksack, suddenly pulling the arm up or down and incorrect positioning during an operation are also possible reasons.
Entrapment of vessels and nerves in the area of the upper thoracic opening (thoracic outlet syndrome) is also a rare cause of shoulder and arm pain. Often there is an additional rib in the neck and the pain can be provoked by certain maneuvers. In addition, shoulder diseases can also cause pain in the shoulder and upper arm. These are, for example, osteoarthritis of the shoulder joint, rotator cuff tear, subacromial syndrome or biceps tendonitis.
In these diseases, the pain is primarily dependent on movements in the shoulder joint. Apart from this, organic diseases can also make themselves felt through pain in the shoulder and neck area. In the first place, the heart attack should be mentioned as an absolute emergency. It shows up in about a third of the typical pain in the left arm, and it often radiates into the shoulder, neck and back. The pain is independent of movement and breath. At the same time, general weakness, anxiety, paleness, sweating, nausea and shortness of breath occur.
In addition, diseases of the liver and biliary tract can cause pain in the right, spleen diseases in the left neck and shoulder region.
Read more on the subject at: Pain in shoulder and arm
causes

Impingement syndrome
In the so-called impingement syndrome, there is a bottleneck in the shoulder joint. Often there is a degenerative change in the tendon of the supraspinatus muscle, which begins to calcify as a result of wear. As a result, it becomes thicker and more rigid, so that it becomes trapped in the roof of the shoulder when certain movements are made. A chronic inflammation of the tendon can also be the cause. This is also seen more often in young athletes who put heavy weight on their shoulder.
Symptoms: Typically, patients report pain when spreading their arm away from the body, especially between 70 ° and 130 °. This area is also known as the painful arc. If the 130 ° is exceeded, the arm can usually easily be raised further, as the shoulder blade then rotates outwards and the shoulder roof opens up the way for the calcified or inflamed tendon.
Diagnosis: The diagnosis of the impingement syndrome can be checked using MRI, CT or ultrasound. These imaging techniques can detect changes in the tendon and shoulder joint so that other possible causes for the symptoms observed can be ruled out. E.g. Check for a tear in the tendon or an injury in the shoulder joint capsule.
If the symptoms improve after the injection of anti-inflammatory drugs into the shoulder joint, the diagnosis of the impingement syndrome can be regarded as confirmed.
Therapy: The therapy is usually carried out by conservative measures, i.e. In most cases, surgery is not performed. First, anti-inflammatory drugs can be injected directly into the shoulder joint; they relieve the symptoms and soothe the irritated tendon tissue.
In addition, a physiotherapeutic treatment is recommended, which should improve and stabilize the mobility in the affected shoulder joint. An alternative method is shock wave therapy (ESWT). Very strong sound shock waves are generated, which can be bundled and directed onto the shoulder. Due to their strong pressure, they are able to shatter calcifications in the shoulder area. The small lime particles can be broken down and removed more easily by the body, so that shock wave therapy can achieve good results.
However, if the pain persists for more than six months despite these measures and is therefore chronic, an operation can be considered. This is usually done arthroscopically, i.e. as part of a shoulder joint specimen. To do this, cameras and instruments are introduced into the joint through small incisions in the skin, so that the areas that have been affected by inflammation can be removed under sight.
Read more on the subject at:
- Pinched nerve on shoulder
- Impingement syndrome
Bruised shoulder
If the pain occurs after a traumatic event, it could be a shoulder contusion. Such an event is typically a shock, a blow, a fall impact, or a collision, e.g. can easily happen during exercise.
Symptoms:
A shoulder bruise manifests itself as pain in the affected area, which is accompanied by redness and swelling. In addition, bruises often occur.
Therapy:
Immediately after the traumatic event, the shoulder should be immobilized and movements paused. It should also be cooled with ice. Compression and elevation (in the case of the shoulder rather relief e.g. through an arm sling) are also good immediate measures. These 4 measures are also known as the PECH rule. In the further course, the healing process can be supported with warming ointments, but you should wait about 2 days. It is important not to put weight on the shoulder until the bruise has completely healed.
Read more about this on our website Bruised shoulder.
Rotator cuff injuries
The rotator cuff is a muscle-tendon plate that is formed by the tendons of the four shoulder rotators and surrounds the shoulder joint.
The muscles involved are:
- Supra- and infraspinatus muscles
- Subscapularis muscle
and - Teres minor muscle.
These muscles ensure the inward and outward rotation of the shoulder joint and stabilize it in its position through the developed tendon plate. This is important because the shoulder joint is only very slightly secured by ligaments and is therefore dependent on increased muscular fixation. Injuries to the shoulder can lead to tendon ruptures in the area of the rotator cuff (rotator cuff rupture).
Symptoms:
If the rotator cuff is only slightly injured, e.g. torn, the pain may be rather minor and not classified as threatening. With a complete tear, however, stronger, mostly load-dependent pain occurs.
Typically, the arm can only be splayed against resistance with pain. As in the case of impingement syndrome, the symptoms are greatest when the angle is between 70-130 ° (painful arc). The inward rotation of the arm is also often associated with discomfort. At night, patients complain of pain when they want to lie on the affected side. Everyday movements can only be carried out with little force or not at all, depending on the extent of the crack.
Diagnosis:
Usually the clinical picture when examining affected patients is characteristic of the diagnosis of rotator cuff rupture. This is especially true for complete demolitions. The drop-arm test, for example, is suitable for checking, in which the doctor spreads the patient's arm away from the body by 90 ° (abducts) and then asks the patient to hold the arm in this position. If the rotator cuff is completely torn off, the patient will not succeed and his arm will simply fall down due to gravity.
In addition, the doctor checks the patient's muscle strength and to what extent it is reduced. This can provide information about the extent of the injury. An MRI or ultrasound scan can also be performed to visualize the injured tendons. In addition, an X-ray image can be made to show the shoulder joint in order to clarify possible causes for the rupture, for example bone protrusions that could have damaged the tendon over a longer period of time.
Therapy:
In the case of injuries to the rotator cuff that only lead to a minor impairment of function, conservative therapy can be tried first. It consists of a combination of anti-inflammatory drugs, pain relievers, and intense physical therapy.
Initially, the shoulder usually has to be immobilized for some time, but physiotherapy should be started early. This is important in order to strengthen the functionality of the shoulder and to maintain its mobility. The training must be carried out consistently for a few months in order to achieve an optimal result.
If these measures do not help or if the symptoms are very severe right from the start, so that the affected arm can hardly or no longer be used, an operation usually has to be carried out. This can often be done arthroscopically, i.e. as part of a joint specimen. The goal of the procedure is usually to sew the torn ends of the rotator cuff together. In addition, annoying bony protrusions that have narrowed the space under the shoulder roof can be removed (subacromial decompression). The bursa lying there is often removed at the same time, as this can also cause severe pain in the shoulder joint when inflamed and additionally narrow the space under the shoulder joint.
For more information on this topic, see our topic: Rotator Cuff Rupture
Osteoarthritis of the shoulder

Osteoarthritis refers to wear and tear on the joints. In Germany, this disease occurs particularly frequently in the knee joint, as it is exposed to particular stress. About 2/3 of all people over 65 years of age are affected by the disease, although the severity can be very different and not all symptoms affected.
One distinguishes one primary from one secondary osteoarthritis. Primary osteoarthritis is based on a cartilage defect for which no precise cause can be assigned. Secondary osteoarthritis occurs as a result of improper stress, overload, previous inflammation of the joint (arthritis) or certain metabolic diseases. The pain typically occurs when the affected joint is stressed. In the course of osteoarthritis, deformities of the affected joints and joint effusions can occur.
Symptoms: Shoulder joint arthrosis usually manifests itself as pain in the shoulder joint that occurs with certain movements. Typically, lifting and spreading the arm, as well as rotating it outward, is painful. Sometimes a grinding or rubbing noise can also be heard in the joint when it is moved. This can be caused by the abraded cartilage.
Diagnosis: The diagnosis is usually made with an X-ray. A narrowing of the joint space is already visible in the relatively early stages of the disease. In advanced stages, the x-ray shows additional bony changes in the joint, e.g. Bony protrusions (Osteophytes) and deformations.
Therapy: Osteoarthritis therapy is initially carried out using anti-inflammatory drugs and intensive physiotherapy to improve mobility. Painkillers can be used to relieve symptoms.
If conservative measures do not help, there are some alternative methods that can be used. There is, for example, the possibility of so-called Chondroprotectives injected into the joint. Chondroprotectives are drugs that are supposed to protect the cartilage from further degradation. Healthy cartilage can also be removed from a less stressed cartilage zone of the joint and transplanted to the main stress points (so-called Autotransplant).
A similar method is that Chondrocyte transplant, in which some cartilage cells are removed from the healthy cartilage. These are grown for a few weeks and then attached to the damaged cartilage. By forming new cartilage, these transplanted cells can compensate for the damage to some extent.
Alternatively come operational procedures in question, especially if the osteoarthritis is more advanced. The joint can either be replaced by a Endoprosthesis replaced or stiffened (Arthrodesis).
An endoprosthesis is a long-term solution, but the joint usually loosens again after about 10 years and then has to be operated on again. For this reason, one would like to avoid inserting an endoprosthesis before the age of 60. The follow-up operations are usually much more complicated than the first operation, as increasingly bone substance is lost and the bone due to aging processes and osteoporotic changes is less resilient.
In arthrodesis (joint stiffening) the corresponding joint is e.g. fixed in one position by screws or wires and can then no longer be moved. This usually results in lasting freedom from pain, but this procedure is also associated with a complete loss of function in the affected joint.
Further information can be found under our topic: Osteoarthritis of the shoulder
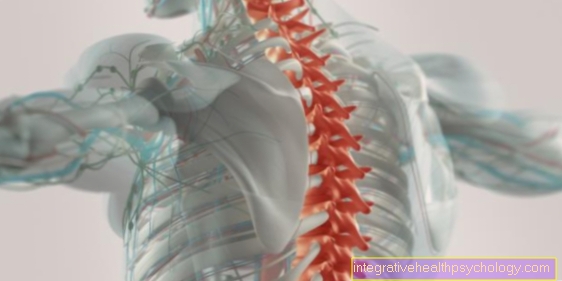
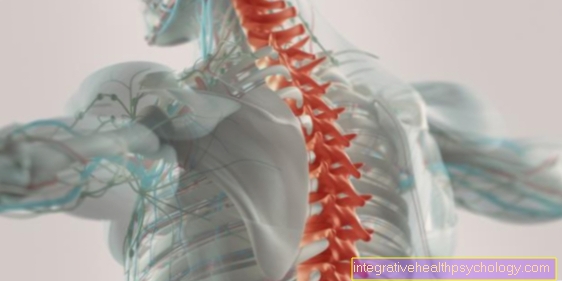
Anatomy shoulder

- Humerus head
- Shoulder height (acromion)
- Shoulder joint
- Collarbone (clavicle)
- Raven bill process (Coracoid)
- Shoulder joint (glenohumeral joint)
Shoulder dislocation
In the Shoulder dislocation it is a dislocation of the shoulder joint. The head of the Humerus It is no longer sitting in the socket, but has slipped out.
With shoulder dislocation, one can traumatic from habitual forms distinguish. The traumatic shoulder dislocation results from the direct application of force (usually on the outstretched arm), whereby the humerus is levered out of its position, e.g. when catching a fall. The habitual shoulder dislocation occurs without previous trauma and is considered to be inherent, e.g. Congenital disorders in the capsular ligament apparatus of the shoulder, muscular malformations or deformities of the shoulder joint, which makes it less stable and consequently more easily luxated.
Symptoms: Different types of shoulder dislocation are described depending on the direction in which the humerus slips. With 90% that is anterior shoulder dislocation the most common. The affected arm is turned outwards and spread apart from the body. The head of the humerus is no longer in the socket, but has slipped forward and down. The patient usually holds the affected arm with the healthy arm. The shoulder dislocation is also very painful.
Diagnosis: Usually it can be determined externally that it is a shoulder dislocation. The doctor can usually already see and feel that the humerus is no longer in its correct position. An X-ray and an MRI can be helpful to rule out injury to bones or ligaments.
Therapy: The humerus must be brought back to its original position. This process is called Reduction. As this can be very painful for the patient, adequate pain therapy must be ensured. Sometimes a short anesthetic may be necessary for the reduction.
At the scene of the accident, you should initially only be cooled and the arm held still. The arm can only be reduced after an X-ray has been taken. A blind attempt at repositioning goes hand in hand with the risk of overlooking a broken bone and injuring vessels, nerves and soft tissue. After the reduction, the arm should be protected for a while.
In addition, subsequent physiotherapeutic treatment is often indicated in order to restore full functionality. Depending on the extent of the slide, the treatment can be lengthy until function and mobility are fully regained.
You can find more information on this topic under our topic: Shoulder dislocation
Frozen shoulder

The so-called frozen shoulder (also: painful frozen shoulder) results in a painful restriction of movement in the shoulder joint. Often the function in the affected joint is completely lost. The frozen shoulder usually occurs in people between the ages of 40 and 60, and in a third of patients on both sides. Men and women are equally often affected by the disease.
The exact causes that lead to the formation of the frozen shoulder have not been clarified. However, it can also arise in the context of previous shoulder injuries, e.g. after injuries to the rotator cuff, a bursitis or an osteoarthritis change in the shoulder joint.
Therapy: The therapy takes place mainly through the administration of anti-inflammatory and analgesic drugs, as well as through intensive physiotherapy. This is to keep the shoulder as mobile as possible. Sometimes mobilization of the shoulder joint under anesthesia is indicated, whereby the stiffened joint is moved forcefully against the stiffening. Cutting (incision) the joint capsule can also help to improve the symptoms.
You can find more information on this under our topic: Frozen Shoulder
Inflammation of the shoulder bursitis (subacromial bursitis)
Pain in the shoulder can also result from the inflammation of the bursa there. This can e.g. happen through overload during sporting activity or through bacterial colonization.
Symptoms: Movements in the shoulder are very painful with bursitis. Often the joint area is also tender on pressure, reddened, overheated or even swollen.
Therapy: As a rule, bursitis heals on its own after a few weeks. Nevertheless, you can get some relief with a few aids. The general rule: Cooling from heat. Heat treatment should be avoided in the case of bursitis. Cold, on the other hand, can improve the pain, for example by applying ice packs. These should be put in a tea towel or similar beforehand. as otherwise they are too cold and can lead to frostbite.
There are also cooling ointments that can also help relieve the pain. In the case of bacterial bursitis, the use of Antibiotics become necessary. In general, the joint should initially be spared and not overloaded with a bursitis.
Further information on this topic can be found at: Bursitis of the shoulder
Shoulder pain with arm pain (cerbicabrachialgia syndrome)

If, in addition to neck or shoulder pain, there is also pain in the arm on the same side, this is known as cervicobrachial syndrome.
The causes of pain that radiate from the neck or shoulder area to the arm usually have their origin in the cervical spine. If there is tension or tilting of the vertebrae due to incorrect posture, incorrect or overloading, this can lead to such symptoms due to compression of the nerves running there. A tightness in the spinal canal (spinal stenosis of the cervical spine) can also cause such complaints, as pressure is exerted on the nerve roots in the narrow bony canal. The corresponding nerves run into the arm and transmit the pain signal accordingly. Another possible cause is a herniated disc in the cervical spine in this area, as the bulging disc can also compress nerves.
Read more on the subject at: Pain in shoulder and arm
diagnosis
A CT, MRI, or X-ray is usually done for referred pain that is suspected to be from the spine. The possible causes of the complaints, such as a herniated disc or spinal stenosis. If the patient already shows pronounced muscle tension in the neck area (Muscle tension), physiotherapy is usually prescribed first. If the symptoms persist, secondary imaging can be used to rule out other causes.
therapy
The appropriate therapy is selected depending on the cause of the symptoms. Initially, treatment is usually attempted with conservative measures. If this is not enough, surgery must be considered, especially in the case of a herniated disc of the cervical spine and spinal canal stenosis. Tension can usually be effectively reduced through physiotherapeutic treatment, massages and relaxation techniques. In addition, care should be taken to maintain an upright posture. To relieve the patient of the pain, mild pain relievers can be administered or injected directly into the tense muscles.
You can find more information on this under our topic: Cervicobrachialgia
Pain in the neck
On the one hand you can Shoulder painthat for example due to inflammation due to overload or a chronic illness, forwarded into the neck become. Through the constant restraintthat is taken because of the pain, it comes to increasing tension of the Neck muscles.
Next Neck pain can also a headache be the consequence. In most cases, if the shoulder pain radiates to the neck, it can be attributed to the pain from the shoulder joint come back.
Upper arm pain

Upper arm pain can use the entire area from the actual shoulder joint to the elbow joint take in. Pain in this area often leads to that even simple movements, such as tightening, can no longer be carried out without complications.
Is the pain in the lateral area of the upper armso this is often a sign of a Inflammation of the bursa in the shoulder joint or for the so-called Impingement Syndrome. Here the long biceps tendonwhich runs through the middle of the shoulder joint between the humerus head and the shoulder roof constricted, What very painful is.
For pain in the front area of the upper arm there is often one Inflammation of the long biceps tendon that runs between the muscles of the upper arm in this area.
At extensive pain In the upper area of the upper arm at the transition to the shoulder, a Inflammation of the shoulder muscle (Deltoides muscle) are available.
Pain in the neck
Pain in the throat can be triggered by shoulder pain. Through the Relieving posture due to the often prolonged pain on the one hand the Neck muscles tense and on the other hand you can get out of it Blockages in the cervical spine area arise.
The other way around, too Cause of the shoulder pain in the Area of the neck lie. At a previous herniated disc in the field of Cervical spine for example can Pinched nerves who continue to pull to the shoulder. In addition to pain, the others can also typical symptoms of a herniated disc of the cervical spine, such as a Numbness, occur.
Shoulder pain at night
Nocturnal shoulder pain are a phenomenon that can be caused by various shoulder diseases and that is based on an anatomical mechanism.
During the day the Joint gap between the humerus head and shoulder roof pulled apart by the weight of the arm, which relieves the surrounding soft tissues. At night, the strong deltoid muscle, which has to fight the weight of the arm almost constantly during the day, pulls the humerus head towards the roof of the shoulder by means of its own tension.
The Associated Narrowing the joint space and compression of soft tissues creates the nighttime shoulder pain. The shoulder behaves in exactly the opposite way to the other large joints, which usually reduce pain at night due to the relief.
A somewhat cumbersome and uncomfortable way to combat shoulder pain is to use a stretching device. The wrist and foot on the side of the painful shoulder are each put in a loop and these loops are connected with a flexible band. In this way, the pull of the arm's weight on the shoulder can be imitated at night.
Alternatively or in addition to this, exercises can be carried out that Deltoid stretch and expand the joint space both in the short term in the event of complaints and as a precaution for a certain period of time.
A simple but effective example is the following exercise: The patient sits on a chair and places his hands under his buttocks. With his back straight and his gaze directed forward, he tilts his upper body to the side opposite the painful shoulder, thereby widening the joint space. This exercise is suitable both for short-term pain relief at night and for regular exercise of the shoulder during the day.
If the pain can only be combated for a short time in the ways shown and recur over several weeks or even increase in intensity, this is immediate Consultation with a doctor to recommend.
Often such nocturnal shoulder pain can be a Early signs of osteoarthritis Its characteristic is that damage that has already occurred can hardly be reversed.
Practically all other shoulder diseases that do not result from a definite injury, such as one, are possible further causes Dislocation of the shoulder or one Biceps tendon tear.
This includes Tension, muscular deficits or so-called bottleneck syndromes. In the latter case, anatomical structures such as nerves and vessels are compressed at certain narrow points, which creates pain that primarily occurs at night due to the mechanism described above.
Connection between different joints
Shoulder pain can various causes to have. Also from pain neighboring areas can radiate into the shoulder. This can just as easily happen the other way around. Shoulder pain can be a basic symptom radiate into the adjacent parts of the body.
The shoulder should not as a single joint but as a unit. To the Shoulder girdle belong to the two Shoulder blades, the Collarbones and the Sternum. There are joints between the bones. If you move one of these joints, you inevitably have Effects on the other jointsthat are passively moved.
That too actual shoulder joint, so the unit of Humerus head and shoulder socket, is not a strictly delimited functional unit.
Besides this joint, there is also that Shoulder joint, so the connection between Shoulder blade and collarbone, and the bearings between the Shoulder blade and ribsthat there is always strain when the arm is lifted.
If you see the shoulder girdle as one Unit of several bones and jointsthat only im Teamwork the full Range of motion It is easy to understand that the pain is mostly too not limited to one of the joints are.
The Nerve plexus, which supplies the muscles and skin of the shoulder, is largely made up of nerves that are in the Area of the cervical spine run away. Therefore this area is also closely related to Functionality and sensitivity connected to the shoulder.
Unfortunately there are many deviations from the norm, so that the assumed self-diagnosis does not necessarily have to be correct. But we hope through our Self-diagnostic just to be able to help the patient on the internet organ or symptom related look for a disease.
Ultimately, however, only a specialist examination and, if necessary, imaging procedures (X-ray image, MRI etc.) lead to the correct diagnosis.
Exercises for shoulder pain
In certain cases of shoulder pain and depending on its cause it can be physical Exercises and training be useful. This is especially the case if the trigger for the discomfort is in Tension due to long-term incorrect shoulder posture or muscular deficits (e.g. after operations and / or immobilization of the shoulder).
However, the suspicion that you are suffering from tension or a muscular deficit can be hide more serious causes of shoulder pain and certain exercises can even make the condition worse.
For this reason it is essential Consult a specialist doctor before deciding on shoulder exercises.
If the doctor thinks it makes sense to exercise, he will usually ask you to Physiotherapists refer to who can teach you the basics of the exercises. This is an extremely important step because if the exercises are done incorrectly, there may be no relief or even one Increase in shoulder pain can be achieved.
Before starting shoulder training, the shoulder can be repeated several times Forward and backward circles be stretched and mobilized (approx. 5-10 times). The effect of this preparation measure is controversial - as is generally the case with stretching the muscles before or after training - but in this case it can be regarded as harmless. The back should be kept straight and the head pointed straight forward.
For further warming up, a simple exercise is suitable, in which the shoulders are pulled up, held there for a few seconds and finally lowered again. Again, this exercise should be done with your back straight and your gaze forward. The exercise is also repeated about 5-10 times.
In general, it can be said that the muscles of the shoulder joint are made up of so many different parts, each with their own tasks, that almost every exercise that includes the Shoulder muscles be addressed.
Since it is not very stressful and easy to dose, the so-called, for example, is particularly suitable Pull-downs with a towel. The patient, sitting on a chair with his back straight and looking forward, holds the two ends of a rolled up towel high above his head with both hands (which should be a little further than shoulder width apart). Now the patient pretends to pull the towel apart and then slowly moves it downwards behind the head. Then he lifts the towel, which is still being pulled apart, back towards the starting position.
This exercise can initially be done in 2-3 sets of 5-10 repetitions each.
Other exercises that target the shoulder muscles to a high degree and thus can be effective against shoulder pain are for example pushups or the Pull-ups. However, these exercises are characterized by a great deal greater stress on the shoulder joint and should therefore only be carried out in moderation after consultation with the expert.
Basically, it should be noted: Success, i.e. pain relief, cannot be achieved from now on, but requires long-term, regular exercise.
Should be an exercise Cause painthe exercise should be stopped immediately.
Even if shoulder pain does not arise during the exercises but afterwards, it should be reassessed together with the expert whether the exercises were adequately selected and performed.
Tap the shoulder joint
The Taping of joints, in this case the shoulder joint, with conventional inelastic tapes should help the patient in two ways: On the one hand, through the one exercised by the tape compression the swelling can be counteracted. In addition, the splinting of the joint achieved by the tape should support the tendons and ligaments in their function.
This is a new kind of taping Kinesio taping. Cotton tapes are used, which are elastic due to the incorporation of elastane threads. Because of this elasticity, it can be seen that neither kinesio tapes Compression one more splint reachable.
There are various hypotheses about the mechanism of action, one of which Activation of the body's own pain-relieving system by irritating skin receptors heard.
Another theory says that by contracting the stretched tape, the underlying skin is lifted and thus an improvement in the Microcirculation as well as the Lymph drainage is achieved. This can have a positive effect on muscle tension and activity.
However, the correctness of these theses and the effectiveness of kinesio taping has not yet been scientifically confirmed.
For both conventional and kinesio tapes, it is advisable to have a professional explain and demonstrate how to put them on correctly. In the case of conventional tapes, in particular, this can prevent improper application of the tape Bad posture which can lead to an exacerbation of the symptoms.
homeopathy
Also the homeopathy states that it has agents that can specifically counteract various causes of shoulder pain.
These means include Arnica and Rhus toxicodendronwhich are said to be particularly helpful for shoulder pain caused by overuse.
rhododendron however, it is recommended for complaints that are intensify in peace.
A classification of shoulder pain according to localization recommends the following homeopathic remedies: for pain of the right shoulder sanguinaria, for the left shoulder Ferrum metallicum and for pain in both Shoulders at the same time Lycopodium.
If you suspect one Calcification process in the shoulder Solanum Malacoxylum Means of choice.
Basically, it must be emphasized that so far there is no reason to consider homeopathic theories as scientifically verifiable. So far, no evidence has been provided that the effect of homeopathic remedies goes beyond the placebo effect. This also applies to homeopathic shoulder pain relievers.
Please note
In no case does the “self” diagnostic agent replace a visit to your trusted doctor! We also make no claim to the completeness of the differential diagnoses presented (alternative causes). We assume no liability for the correctness of the self-diagnosis you have made! We strictly reject any form of self-therapy without consulting your doctor!
To the diagnostic
Using our “Self” diagnostic agent is simple. Follow the respective link offered, where the location and description of the symptoms best match your symptoms. Pay attention to where the Shoulder joint the pain is greatest.
Medical terms on the subject of shoulder
For the exact anatomical assignment, we refer to the Anatomy Lexicon our page.
Here are some important location names:
- dorsal - back
- ventral - front
- medial - inside
- lateral - outside, laterally
Where is your pain?
For orientation purposes, shoulder pain can be divided into anterior and posterior shoulder pain, which is based on typical diseases due to the anatomical structure of the shoulder joint.
Within the more common anterior shoulder pain, acute shoulder pain can be distinguished from chronic shoulder pain.
The most common reason for acute anterior shoulder pain is a dislocation, i.e. a dislocation of the shoulder joint. In about 80-90% of shoulder dislocations, the humerus head slips forward and down out of the joint socket and compresses the surrounding structures there, which causes severe pain.
A rare cause of acute pain in the right shoulder area can, surprisingly, also be a gallstone. Due to certain nerve connections, the pain radiates from the abdomen into the shoulder.
Chronic shoulder pain is more difficult to discuss because it can result from a wide variety of pathological processes. Inflammations of the bursae, which are mainly located in the front, are particularly frequent here, i.e. bursitis (Bursitis). Since this is an inflammation, the pain is often accompanied by redness and swelling, which can help distinguish it from the other causes of anterior shoulder pain.
Other causes of anterior shoulder pain can be degenerative changes in muscles or tendons, which can lead to muscle or tendon tears, whereupon the chronic pain develops into acute pain.
Read more on the subject at: Front shoulder pain
In the case of back shoulder pain, acute and chronic complaints must also be distinguished. Acute back shoulder pain is often caused by a vertebral block in the thoracic or lumbar spine. In addition to restricted mobility, a characteristic feature is the radiation of the pain from the spine to the back shoulder.
Chronic pain in the back shoulder area can be caused by an impingement syndrome. It is typical for this that the patient feels severe pain when lifting the extended arm to the side, especially between 60 and 120 ° ("painful arc"). Chronic pain can turn into acute when a degenerated tendon of the supraspinal muscle tears.
Read more on the subject at: Back shoulder pain
Finally, there are diseases that can trigger anterior, posterior or global pain in the shoulder joint.
This includes muscular tension, which, depending on where it occurs, can cause pain in the anterior or posterior shoulder joint (e.g. as a result of herniated discs or shoulder blade misalignments).
Osteoarthritis, on the other hand, often triggers centrally located shoulder pain with particularly painful areas (depending on which partial shoulder joint is affected).
Front shoulder pain

Front shoulder pain usually relates almost exclusively to pain in the area of the front shoulder joint.
In addition to pain in the area of the anterior rotator cuff and the biceps tendon, this also includes pain in the area of the shoulder joint (AC joint) and the collarbone (clavicle).
Anterior shoulder joint pain can be caused by direct damage to the specific anatomical structures, but can also originate from a more distant anatomical area and thus appear as "transmitted pain".
For more information, see: anterior shoulder pain
Back shoulder pain
Back shoulder pain mainly refers to pain in the area of the back of the shoulder joint. The pain in the area of the rear shoulder joint includes problems in the area of the rear rotator cuff and cervical vertebra blockage, thoracic vertebra blockage, herniated discs in the cervical spine and disorders in the movement of the shoulder blade (scapula).
Just like anterior shoulder joint pain, pain in the area of the posterior shoulder joint can cause direct damage to the anatomical structures involved. However, the cause can also be found in a more distant part of the body.
For more information, see: back shoulder pain or pain under the shoulder blade
Figure shoulder muscles

Shoulder muscles
- Scapula-hyoid bone muscle -
Omohyoideus muscle - Anterior stair muscle -
Scanelus anterior muscle - Head turner -
Sternocleidomastoid muscle - Collarbone - Clavicle
- Deltoid - M. deltoideus
- Raven bill process upper arm muscle -
Coracobrachialis muscle - Subscapular muscle -
Subscapularis muscle
(second layer) - Two-headed upper arm muscle
(Biceps) - M. biceps brachii - Pectoralis major -
Pectoralis major muscle - Scapula lifter -
(second layer) -
Muscle levator scapulae - Upper bone muscle -
Muscle supraspinatus (second layer) - Scapula bone -
Spina scapulae - Small round muscle -
Muscle teres minor - Subbone Muscle -
Muscle infraspinatus - Large round muscle -
Muscle teres major - Trapezius -
Muscle trapezius - Broad back muscle -
Muscle latissimus dorsi
Rotator cuff
= 4 muscles (7th + 11th + 13th + 14th) -
covered by the deltoid
You can find an overview of all Dr-Gumpert images at: medical illustrations