Joints
Synonyms
Joint head, joint socket, joint mobility,
Medical: Articulatio
English: joint
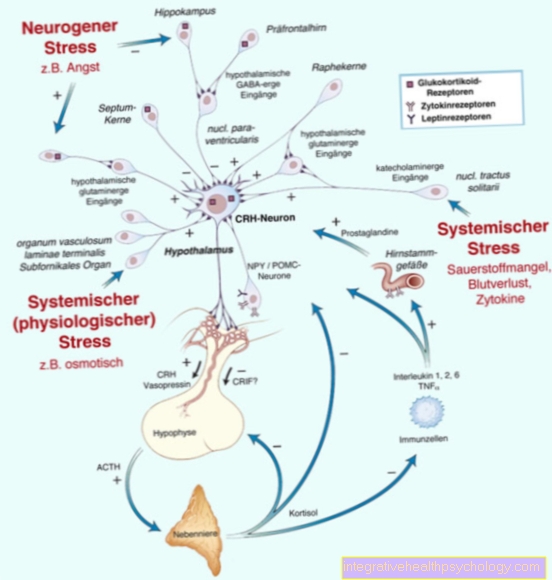
Figure joint shapes

- Wheel angle joint
= Swivel hinge joint
(e.g. knee joint) - Saddle joint
(e.g. thumb saddle joint) - Ball joint
(e.g. shoulder joint,
Hip joint) - Hinge joint
(e.g. elbow joint) - Wheel joint
= Pivot joint
(e.g. spoke-ulnar joints) - Egg joint (not shown)
similar to ball joint,
only biaxial
(e.g. proximal wrist)
Uniaxial Joints -
Hinge joint and wheel joint
Biaxial joints -
Wheel angle joint, saddle joint
and egg joint
Triaxial joint - Ball joint
You can find an overview of all Dr-Gumpert images at: medical illustrations
Appointment with ?

I would be happy to advise you!
Who am I?
My name is I am a specialist in orthopedics and the founder of and work as an orthopedist at .
Various television programs and print media report regularly about my work. On HR television you can see me live every 6 weeks on "Hallo Hessen".
But now enough is indicated ;-)
In order to be able to treat successfully in orthopedics, a thorough examination, diagnosis and a medical history are required.
In our very economic world in particular, there is not enough time to thoroughly grasp the complex diseases of orthopedics and thus initiate targeted treatment.
I don't want to join the ranks of "quick knife pullers".
The aim of all treatment is treatment without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You will find me:
- - orthopedic surgeons
14
You can make an appointment here.
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
For more information about myself, see - Orthopedists.
Types of joints
Joints are divided into real joints (Diarthrosis) and fake joints (Synarthroses). The real joints are separated from one another by a joint space. If the joint space is missing and filled with filling tissue, it is called a fake joint.
In the case of the false joints, between the
- banded (Syndesmoses),
- cartilaginous (Synchondroses) and
- bony (Synostoses) differentiated.
False joints
Fake joints (Synarthroses) usually only allow a small amount of movement, although this depends on the type of filling fabric. Ligamentous joints are subjected to tension and cartilaginous ones to pressure. Bony fake joints are only created by constant movement at the ossification (Synostosis) prevented.
- In the band-like fake joints (Syndesmoses) two bones are connected by tight, collagen-fibrous connective tissue, rarely also by elastic connective tissue.
These include the interbone membranes between the forearm and lower leg bones (Membranae interossea antebrachii et cruris), the ligamentous apparatus of the distal tibial-fibula joint (Syndesmosis tibiofibularis) and the ligament connections of the spine.
The connective tissue membranes between the cranial bones of a newborn (Fontanelles) are also among the Syndesmoses. - For cartilaginous fake joints (Synchondroses) the intermediate tissue consists of articular cartilage (hyaline cartilage). These include the connection between the bony Diaphysis and the Epiphysis of a youthful long bone, the former connections between the bony parts of the hipbone and the costal cartilage between the ribs and the sternum. The intervertebral disc and the pubic symphysis are also included.
- In the bony fake joints, individual bones are connected secondarily by bone mass. These include the ossified sacrum (Sacrum), the hip bone (Os pelvis) and also the ossified epiphyseal plates of the long bones in adults.
Real joints
All real joints consist of two bones, the articular surfaces of which (Articular facies) are covered with hyaline articular cartilage. This layer differs in its thickness between the individual joints and is dependent on the mechanical load.
Hyaline articular cartilage is usually bluish milky. Due to the absence of the cartilage membrane (Perichondrium) this has a reduced ability to regenerate and is also only nourished by diffusion and convection via the synovial fluid. In doing so, the cartilage becomes thinner through loading and unloading in stressed areas and when relieving it absorbs the synovial fluid like a sponge. Four zones in the direction of the bone are distinguished within the hyaline articular cartilage.
4 zones of the hyaline articular cartilage:
- Zone 1 is the tangential fiber zone. Its main purpose is to reduce shear and friction forces.
- The transition zone is zone 2,
- the radial zone is the 3rd zone, which is the dividing zone between the non-mineralized and mineralized cartilage.
- The 4th zone is the mineralization phase, which forms the transition between bone and cartilage.
The joint space or the joint cavity is located between the two joint partners. The joint cavity is the part within the joint capsule where both joint partners no longer have direct contact with one another. The shape of the joint cavity changes with the movement of the joint.
This is with synovial fluid (Synovial fluid), which on the one hand is responsible for nourishing the joint cartilage and on the other hand absorbs mechanical stress. The joint is surrounded by the joint capsule. This membrane consists of two parts,
- the membrana fibrosa and the
- Synovial membrane.
The Membrana fibrosa consists of tight, collagen-fibrous connective tissue that is located in the periosteum (Periosteum) of the respective bones involved in the joint. In numerous joints the Membrana fibrosa through internal ribbon-like structures (Ligg. capsularia) reinforced. They are responsible for the stability and guidance of the joints.
particularities
In certain joints there are additional structures within the joint (intra-articular structures) in front.
Articular menisci are sickle-shaped structures that are wedge-shaped in cross-section are only found in the knee joint. They consist of tight collagen connective tissue and fiber cartilage. They serve to compensate for the joint partners that are not designed to fit properly and to reduce the pressure load on the articular cartilage.
Articular disc are disc-shaped and partly made of connective tissue, partly made of fiber cartilage. They divide a joint into two separate chambers and reduce the pressure load on the fibrous cartilage.
They occur in the temporomandibular joint, in the collarbone joint and in the wrist near the body.
Joint lips
Joint lips (Labra articularia) of the joints are wedge-shaped deposits on the edges of the bony hip and shoulder joint sockets. They mainly consist of fiber cartilage and are fused with connective tissue on the outside of the joint capsule. The joint lips enlarge the joint surfaces. Intra-articular ligaments are also known as intracapsular ligaments, occur in the knee and hip joint and have different functions. While the cruciate ligaments (see also cruciate ligament tear) (Ligg. cruciata) perform a predominantly mechanical task in the knee, the femoral head band (Lig. Capitis femoris) as a vascular ligament to nourish the femoral head. They consist of tight, vascularized connective tissue and are covered by parts of the synovial membrane.
Joint mobility
The movement behavior of the joints is measured with the help of the theory of movement (kinematics) described.
Every joint movement is traced back to two basic movements and is therefore always a compound complex movement.
On the one hand there is a:
- Sliding or sliding movement of the joints (Translational movement), on the other hand one
- Rotational movement of the joints (Rotational movement).
When sliding or sliding, a body moves on a straight line or on any curved curve in space. Here the body does not turn around itself. So all points of the body make the same movement. The movement can take place along three spatial axes. One speaks here of three degrees of freedom of the displacement movement. If one or two main directions are blocked in a joint, the number of possible directions of movement is reduced.
When the joints rotate, a joint body rotates around an axis or a center point. The pivot point can be inside or outside the joint. Here, too, three degrees of freedom are possible. During the rotary movements, the joint surfaces can slide or roll over one another, with a combination of rolling and sliding usually taking place.
When a joint body moves on its joint surface with the axis gain travel, one speaks of rolling. However, if a body rotates without gaining travel on its axis, but gaining travel on its surface, sliding occurs.
Shoulder joint
- Flexion 170 °
- Extension 40 °
- Approach 30 °
- Spreading 160 °
- Inward turning 70 °
- Outward turning 60 °
Elbow joint
- Flexion 150 °
- Extension 10 °
wrist
- Flexion 60 °
- Extension 40 °
- Approach 30 ° (radial duction)
- Spreading 40 ° (ulnar deviation)
- Inward rotation 90 ° (pronation)
- Turning outwards 90 ° (supination)
Finger joints
- Flexion 90 °
- Extension 0 °
hip joint
- Flexion 140 °
- Extension 10 °
- Approach 30 °
- Spreading 50 °
- Inward turning 50 °
- Outward turning 40 °
Knee joint
- Flexion 150 °
- Extension 10 °
- Inward turning 10 °
- Outward turning 40 °
Upper ankle
- Flexion 50 °
- Extension 30 °
Lower ankle
- Inward turning 20 ° (inversion)
- Outward turning 10 ° (eversion)
Greeting toe joint
- Flexion 45 °
- Extension 70 °
Shoulder girdle
- Take up 40 °
- Pull down 10 °
- Pull forward 30 °
- pull back 25 °
Overview of all important joints
Shoulder joint
The Shoulder joint (Latin Articulatio humeri) is derived from the uppermost part of the Humerus, also called humerus head (Latin Caput humeri), and the joint socket of the Shoulder blade (Latin: Scapula), also Cavitas glenoidalis, formed. It is that most agile but also at the same time most vulnerable Joint of the human body.
But where does the great mobility of our shoulder joint come from? The Articular surface of Humerus head is about three to four times larger than the articular surface of the Shoulder blade. This pronounced disproportion allows great freedom of movement.
At the same time, however, the decreases stability, since there is no firm, bony guide. So it is not surprising that about 45% all Dislocations (Joint dislocation) fall on the shoulder.
From a systematic point of view, the shoulder joint is one of the Ball joints. It is named after the almost spherical shape of the humerus head. The shoulder is a typical representative of this type of joint three degrees of freedom, so six possible directions of movement.
In addition to the bones involved are also Tapes, Bursa, Joint capsule and Muscles involved in joint formation. The structures mentioned are primarily responsible for the movements of the shoulder. They also have the important task of stabilizing the joint! For example, the ligamentum coracoacromiale together with bony parts (Latin acromion and processus coracoideus) form the "Shoulder roof“And so limits upward movements (cranial).
In addition, the strong shoulder muscles secure the joint! The most important muscle group is the so-called "Rotator cuff". To her belong the Infraspinatus muscle, M. supraspinatus, M. teres minor and the M. suprascapularis. They encompass the shoulder from several sides and are largely responsible for stabilization.
This is a common shoulder injury Impingement syndrome, also called painful arch: when the arm is spread sideways (Abduction) between 60 and 120 degrees, those affected feel great pain. A calcified and thickened one is responsible Tendon of the supraspinatus muscle. When the arm is raised, it moves under a protruding bone and a bursa (lat. Finally, the tendon hits (English to impinge = to push) with increasing movement and is painfully constrained.
Elbow joint
The elbow joint (Latin articulatio cubiti) is formed by the humerus (Latin humerus) and the two forearm bones ulna (Latin ulna) and radius (Latin radius). Within the joint, three sub-joints can in turn be distinguished: the humerus joint (Latin art. Humeroradialis), the humerus joint (Latin.Art. Humeroulnaris) and the proximal ulnar spoke joint (art. Radioulnaris proximalis) (see below). These three individual joints form a functional unit and are enclosed by a common, delicate joint capsule. Fan-shaped lateral ligaments, also called collateral ligaments, stabilize the joint and strengthen the capsule. Furthermore, the ring ligament (lat. Lig. Annulare radii) supports the bony guidance in the proximal ulnar spoke joint.
In its entirety, the elbow joint enables bending and stretching movements (flexion and extension), as well as rotating movements (pronation and supination) of the forearm. For many fine motor activities of the hand, such as turning a screwdriver, unlocking a door lock or bringing food to the mouth, the ability to turn the forearm is of great importance!
1) Upper arm joint
The humeral joint of the humerus is formed by the joint role of the humerus, the trochlea humeri, and a depression in the ulna, the incisura ulnaris. From a functional point of view, it belongs to the group of hinge joints and enables the forearm to be bent and extended.
2) upper arm spoke joint
In this joint, a small cartilage surface of the upper arm, also called humerus head or capitulum humeri, articulates with a depression in the radius, also known as the fovea articularis radii. From a purely form point of view, it is one of the ball joints. However, a connection of connective tissue between the two forearm bones (membrana interossea antebrachii) severely restricts the movements! This means that there are only four directions of movement instead of the usual six.
3) Proximal ulnar spoke joint
The proximal ulnar spoke joint is a swivel joint, more precisely a pivot joint. On the inside, the strong ring band is covered with cartilage and is in contact with the joint surfaces of the ulna and radius!
wrist
The term "wrist“Sums that up colloquially proximal radiocarpal joint as well as the connection between two rows of Carpal bones, the Mediocarpal joint, together. Often a simple distinction is made between “proximal” (close to the body) and “distal” (far from the body) wrist. The tasks and functions of our hand are also complex, similar to the structure of the two partial joints!
1.) Radiocarpal joint
Put simply, the radiocarpal joint connects the Forearm bones with the Carpal. The distal end of the radial bone, the articular disc (cartilage surface), and three bones of the proximal wrist (navicular bone, moon bone, triangular bone) form the connection. If you look at the shape of the articular surfaces, the radiocarpal joint belongs to the group of Egg joints. It thus has two axes of motion and four Possible directions of movement: flexion and extension (palmar flexion and dorsiflexion), as well as lateral spreading inwards or outwards (radial / ulnar abduction).
2.) Mediocarpal joint
Between the proximal (scaphoid, moonbone, triangular bone) and distal carpal row (large and small polygonal bone, head bone, hook bone) runs roughly S-shaped joint space. Two at a time opposite bones form a Single joint. In their entirety, they are called the mediocarpal joint. Functionally it belongs to the Hinge joints. However, through numerous ligaments it is in its movements highly limited. It also interacts with the radiocarpal and intercarpal joints. This is why the doctor also calls this joint "interlocked“Hinge joint.
The ligaments of the carpal bones mentioned above are of particular importance. In the case of carpal injuries, for example a scaphoid fracture, they are often also affected. Elderly people also often suffer from wear-related pain, for example in the cartilage (discus articularis) of the radiocarpal joint.
Finger joints
Our fingers are made with the exception of the Thumb made of three small bones each: Phalanx (Latin phalanx proximalis), Phalanx (Latin Phalanx media) and Distal phalanx (Latin phalanx distalis). They stand one below the other through one articulated connection in contact. So we find it in every finger except the thumb three Single joints. Fine motor and complex movements are possible! Since the thumb has no middle link, it only has two Joints.
First of all, that connects Metacarpophalangeal joint (Latin Art. metacarpophalangealis) the respective metacarpal bone with the phalanx. That is what follows Mid-finger joint (Art. Interphalangealis proximalis) between the phalanx and the middle phalanx as well as the Finger joint (Art. Interphalangealis distalis) between the middle and terminal phalanx.
From a purely form perspective, the basic joint is one of the Ball joints. However, there is the third axis of motion, namely the rotation or respectively rotation, strong through the side ligaments limited. Ultimately, the fingers can be flexed and stretched in the metatarsophalangeal joint and spread on both sides.
To make the cumbersome Latin naming of the two remaining joints easier, doctors simply abbreviate the long names: the middle finger joint becomes too PIP, the wrist toe DIP. Both are pure Hinge joints with an axis of motion and thus two possible movements (flexion and extension).
On the underside of the wrist, the tendons of the long finger flexors each run in a joint Tendon sheath. This is in turn attached to the bony finger bones by ring and cruciate ligaments. In addition, the individual finger joints are through Sidebands (Latin ligg.collateralia) supported. What makes them special: they are relaxed when the fingers are in the extended position, whereas they are tensed when they are bent. At Plaster casts The fingers must therefore be in the hand slight flexion be fixed! Otherwise the collateral ligaments will quickly regress and shorten. In the worst case, flexing is no longer possible afterwards.
Knee joint
Our knee joint (Art. Genu) consists of two partial joints. On the one hand, the thighbones (lat. Femur) and shins (lat. Tibia) form the femorotibial joint. Furthermore, the kneecap (lat. Patella) and thigh articulate in the femoropatellar joint. Both partial joints are surrounded by a common capsule and represent a functional unit.
In its entirety, it is a hinge joint with possible flexion, extension and internal and external rotation.
If you stretch the knee joint, you can also observe the special feature that gives it its name: When exercising maximum movement, the lower leg turns slightly outwards (“final rotation”).
Numerous structures ensure the stability and resilience of our knee:
Cruciate ligaments
The anterior cruciate ligament (Lig. Cruciatum anterius) and posterior (Lig. Cruciatum posterius) stretch within the joint capsule. Both ligaments secure the contact between the shin and thigh and provide stability, especially during turning movements. When the cruciate ligament is injured, patients therefore often experience significant uncertainty or instability in the knee joint.
Menisci
It is named after the crescent-like shape (lat. Meniscus = crescent) of the two cartilage structures. They enlarge the joint surface and thus ensure an even load. We differentiate between the outer and inner meniscus, whereby the inner meniscus is closely fused with the joint capsule and the inner knee ligament. Accordingly, the inner meniscus is affected far more often in injuries!
Sidebands
The colloquially known "inner ligament" (Latin. Lig. Collaterale tibiale) runs on the inside of the knee joint. Accordingly, the so-called "outer ligament" (Latin. Lig. Collaterale fibulare) can be found on the outside. They prevent our knee from buckling to one side. It is therefore only logical that the collateral ligaments are injured primarily during lateral twisting movements. If both the inner ligament, the inner meniscus and the anterior cruciate ligament tear, one speaks of an "unhappy triad".
hip joint
Our hip joint (lat. Art. Coxae) represents the articulated connection between the upper body and legs. On the one hand, it enables walking and standing upright, and on the other, it ensures stability in the middle of the body!
The femoral head, also called the femoral head, (lat. Caput femoris) and the cartilage-covered hip socket (lat. Acetabulum) form the bony parts. The latter is the result of the fusion of the iliac bone (lat. Os ilium), seat bone (lat. Os ischii) and pubic bone (os pubis).
The hip joint is a special form of the ball joint, namely a nut joint with three axes of movement. Thus, flexion and extension, internal and external rotation as well as lateral spreading are possible here.
Characteristic are the strong and massive ligaments which press the spherical femoral head together with the tight joint capsule firmly into the socket. In this context, the doctor often speaks of a “ligament screw” (iliac-thigh ligament, ischium-thigh ligament and pubic-thigh ligament).
For example, the iliac-thigh ligament has a tensile strength of over 350 kg and is therefore the strongest ligament in the human body! When standing upright, it also prevents the pelvis from tilting backwards without the use of muscle power. Another special feature of the hip joint is the femoral headband. Blood vessels run in it, which are extremely important for the supply of the femoral head. It plays a huge role in curing femoral neck fractures.
Often the hip joint shows signs of wear and tear with increasing age, the so-called coxarthrosis. Experts now assume that around 2% of all 65-74 year olds in Germany are affected. Overweight patients without sufficient exercise are particularly at risk. As the disease progresses, pain and inability to move in the hip joint increase. In the worst case, an endoprosthesis (“artificial hip”) is the only therapeutic solution.
Ankle
This is what the colloquial term "ankle" means upper (Art. Talocruralis) and lower ankle (Art. Subtalaris and Art. Talocalcaneonavicularis). Many small Tarsus and Tapes act with one another in a very complex manner and thus enable, among other things, to walk upright.
Upper ankle
Both ends of the lower leg bones distant from the body Shin and Fibula form the so-called Malleole fork, also called ankle fork. It embraces the on both sides Joint roller (lat. Trochlea tali) des Talus and thus forms the upper ankle joint. The pure Hinge joint thus connects the lower leg and tarsus and enables flexion and extension.
The joint has on the one hand for stabilization and movement control Sidebands (Interior and Outer bands) between the lower leg bones and the tarsus. Second, the tibia and fibula are through the Syndesomal ligaments connected with each other.
Injuries to the upper ankle are extraordinary often. Typically, those affected bend outwards on uneven ground (suppination trauma). This primarily results in overstretching or even tears in the outer band. Colloquially, the term "sprain“Enforced.
Lower ankle
Within the lower ankle joint, a distinction is made between an anterior and a posterior partial joint. In the anterior lower ankle joint form various Tarsus (Heel bone, scaphoid bone) as well as the one covered with cartilage Pan band a joint socket for the talus (lat. Talus). In addition, the pan strap strengthens ours Longitudinal arch of the foot.
The posterior lower ankle is made up of the Ankle bone and the Calcaneus (lat. Calcaneus) together. The ankle-calcaneus ligament (lat. Lig. Talocalcaneum interosseum) runs between the two chambers of the lower ankle joint and thus forms the spatial dividing line.
The range of motion in the joint is similar to that in the upper ankle a Axis of movement: With the ankle bone fixed from the front, the heel can be turned inwards (inversion) as well as outwards (eversion). Ultimately, however, it is difficult to reduce the movements in the foot to individual joints. Because almost all components within the foot are coupled to one another, so that movements are usually carried out in combination.
Toe joints
Colloquially, all joints of the toe bones fall under this term. Their structure is very similar to that of the finger joints.
According to this, every toe, with the exception of the big toe, consists of three small bones: Basic link (Latin phalanx proximalis), Middle link (Latin Phalanx media) and End link (Latin phalanx distalis).
We find them between the individual heads of the metatarsals and the base limbs of all toes Metatarsophalangeal joints (Latin art. metatarsophalangea). This is followed by between reason- and Middle link, the mid-toe joint (art. interphalangealis proximalis, PIP).
Like the thumb, the big toe consists of only reason- and End link. Since she does not have a middle link, the corresponding middle toe joint is also missing!
On all toes, however, that connects End joint (Latin. Art. interphalangealis distalis, DIP) middle / base and end phalanx. In some people, the last two bones of the little toe are fused together.
In summary, there are five metatarsophalangeal joints, four central toe joints and five end-toe joints.
From a functional point of view, the joints between the toe bones are among the Hinge joints. It allows us to bend and straighten our toes. This ability is an important requirement when walking and running.
Numerous ligaments, tendons and muscles support the complicated anatomy.
Typical complaints of the toe joints can be, for example, in the context of Malpositions of the feet appear. Especially with the clinical picture of Splayfoot the base joints of the toes II-IV cause discomfort. The typical loss of the transverse arch of the foot creates an increased pressure load on the head of the. In addition, the small toe joints are not uncommon with age arthrosis affected.