thyroid
Synonyms
- Thyroid lobe
- cold knot
- warm knot
- hot knot
- cyst
- Thyroid tumor
- Graves disease
- Hashimoto's thyroiditis
Medical: Glandula thyroidea
English: thyroid glands
definition
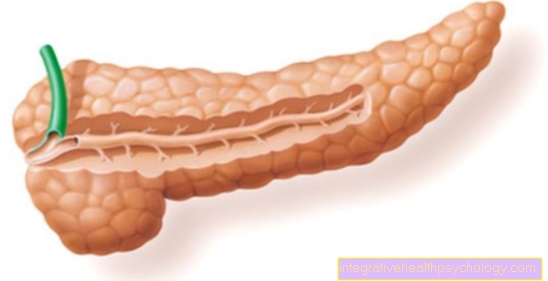
Thyroid (Glandula thyroidea) is an unpaired gland, which is located on the neck below the larynx. It consists of two lobes connected to one another via the so-called isthmus, which extend on both sides of the neck. This makes it resemble a shield; therefore the name. It is called a gland because it Manufactures and releases hormones. Their primary job is to Regulation of the energy metabolism and growth. At the back of the thyroid gland, humans still have so-called parathyroid glands, which, however, are to be distinguished from the thyroid gland.

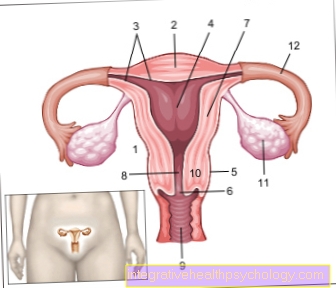
Illustration of the thyroid

thyroid
- Hyoid bone -
Hyoid bone - Thyroid cartilage
Hyoid bone membrane -
Thyrohyoid membrane - Thyroid cartilage -
Cartilago thyroidea - Cricoid cartilage
Thyroid cartilage muscle -
Cricothyroid muscle - Upper parathyroid -.
Parathyroid gland
superior - Thyroid constriction -
Isthmus glandulae
thyroideae - Thyroid,
right lobe -
Glandula thyroidea,
Lobus dexter - Lower Parathyroid -.
Parathyroid gland
inferior - Trachea - Trachea
You can find an overview of all Dr-Gumpert images at: medical illustrations
Thyroid anatomy
The 20 to 25g heavy in adults thyroid belongs to the so-called endocrine organs of the body. Their main (endocrine) task is the formation of hormones that are released (secreted) into the blood.
It is made up of two lobes on both sides of the windpipe (Trachea) and the overlying cartilage of the Larynx (Larynx). Accordingly, this larynx cartilage is called thyroid cartilage. In men, it shows as a protrusion on the neck, the Adam's apple. The connecting piece between the two lobes is the so-called isthmus.

Anatomy of the neck / larynx
- throat
- Thyroid cartilage of the larynx
- thyroid
- Windpipe (trachea)
There is also the so-called parathyroid gland. The parathyroid glands are four lens-sized glands weighing approx. 40 mg. They lie behind the thyroid gland. Sometimes an additional parathyroid is also found.
The parathyroid gland produces an important hormone (parathyroid hormone) that regulates the calcium balance.

Anatomical structure of the thyroid gland
- Thyroid lobes
- Connecting piece (isthmus)
Thyroid function
The main task of the thyroid is to regulate the energy metabolism. To do this, it produces two hormones that regulate the basal metabolic rate, i.e. the energy generated under resting conditions: thyroxine (T4 for short) and triiodothyronine (T3 for short).
They are not only released into the blood depending on the hormones, but are also stored within the organ in so-called follicles. The follicles are cavities enclosed by flat surface cells (epithelial cells). However, these are not filled with biologically active hormone, but contain a precursor of the hormone that is easier to store, thyroglobulin. The same is also known as a colloid, formed by the thyroid cells and then released inwards into the cavity. From these large protein molecules (thyroglobulin), the required amount of hormone is then cut out by means of enzymes and released into the bloodstream.

Structure of the thyroid gland under the microscope
- Epithelial cells (flat)
- Filled follicles (thyroid follicles with thyroglobulin)
The main component of thyroid hormones is iodine, which is taken up as a negatively charged ion, i.e. as iodide, into the epithelial cells of the thyroid gland and the amino acid tyrosine is coupled.
4 iodine atoms are required for thyroxine (hence it is also called tetraiodothyronine or T4; Greek tetra = four), however, for triiodothyronine, T3 hormone, only three iodine atoms.
T4 represents the hormone primarily produced by the thyroid gland, which, however, is ten times more effective in the target tissues T3 is converted. This task is carried out by an enzyme called deiodase, which removes one iodine atom from the tyrosine at a time. T3 itself is only produced in small amounts by the thyroid gland itself. The size of the cells surrounding the thyroid follicle and the filling level of the follicle reflect the activity of the entire organ. A lot of hormones are needed in childhood, so the follicles are small, poor in colloids and lined with large epithelial cells. This is the hormone that stimulates the thyroid gland to grow and release hormones (Thyroidea stimulating Hormon, short TSH), which is formed by the hypothalamus (part of the brain) and reaches the thyroid through the bloodstream.
On the other hand, large amounts of hormones are stored in old age and the thyroid follicles contain a lot of colloid. (Less hormone is needed; in older people the energy requirement decreases accordingly.) Due to the increased energy requirement, both cold and pregnancy have an activating effect on the thyroid gland; Heat tends to have an inactivating effect.
Another function of the thyroid is to regulate the calcium level in the blood. Specialized cells, which are scattered between the follicle cells, produce the hormone for this Calcitonin. This small hormone lowers the level of calcium in the blood by reducing the build-up of Calcium promotes into the bones. So it works osteoporosis opposite. It also inhibits the cells that are naturally responsible for breaking down bone tissue (and thus avoid excessive ossification in the body), as these too can contribute to an increased calcium level in the blood. Another mechanism of Calcitonin consists in promoting the excretion of calcium via the Kidneys.
Which doctor treats the thyroid?
Since the thyroid is a hormone-releasing gland, the doctor who is most familiar with the thyroid is the so-called endocrinologist. He is particularly concerned with the Hormones, their control systems and their glands.
The endocrinologist may be able to do one Specialist in nuclear medicine instruct to determine the hormone-producing activity of the tissues; the so-called Thyroid scintigraphy. This is suitable for finding areas of the thyroid gland that may be overactive or no longer active.
However, if there is a need to remove all or part of the thyroid gland, the general surgeon is the one to perform the operations.
Thyroid hormones
This is what the so-called thyroid hormones mean Triiodothyronine (T3) and that Thyroxine (T4). These differ in whether three (T3) or four (T4) iodine atoms are bound to the hormone molecule.
Thyroid hormones affect the entire body through the Binding to special receptors out. Generally they work stimulates the metabolism and generating heat (thermoregulating) by increasing energy expenditure and also increasing breathing rate. They also have a stimulating effect on the heart, increasing the pulse and strength of the heart to a certain extent. Also constructive (anabolic) Metabolic pathways, such as Muscle building is stimulated, whereby an overdose also has the opposite effect. They also play a major role in the child's growth phase Body and skeletal growth and also one in the maturation of the nervous system.
The thyroid hormones also have a stimulating effect on all other cells in the human body, e.g. on the skin and hair or the gastrointestinal tract.
This also results in the Symptoms of a deficiency or an excess. A defect like the one with one Hypothyroidism (Hypothyroidism) occurs, can manifest itself, for example, in internal weakness, weight gain, sensitivity to cold (due to less heat production), a low pulse and dry, rough skin. An excess, such as a Hyperthyroidism (Hyperthyroidism) can manifest itself in an increased pulse, damp and sweaty skin, inner restlessness and nervousness.
In the thyroid gland the hormones are attached to a carrier protein (Thyroglobulin) bound manufactured and stored. If necessary, these are then mobilized from the storage reserves and released into the bloodstream.
Because the thyroid hormones poorly soluble in water are, they are also bound to carrier and transport proteins in the blood (Serum albumin, TBG, transthyretin). However, only those parts of the blood that are not bound are really hormonally effective, whereby these make up the smallest part (less than 1%).
The release of the two thyroid hormones is not in equal proportions, but rather in the ratio of 20% T3 and 80% T4. However, so-called T3 is predominantly biologically effective. The T4 practically serves as an existing reserve, since the T3 is broken down much faster (T3 half-life: approx. 1 day, T4 half-life approx. 1 week). The T4 is then converted into the more biologically active T4 by certain enzymes, so-called deiodases. The T3 can therefore be viewed as a kind of depot form of the T4.
In the laboratory determination, the so-called TSH is often determined as a substitute for the thyroid hormones. This laboratory value is good for estimating the body's need for and coverage of thyroid hormones.
Causes of an enlarged thyroid / thyroid swelling

A thyroid gland that is too large can be found in 30% of adults in Germany. Regardless of the cause of the thyroid enlargement, one then speaks of a goiter, colloquially also as "Goiter“, But there are also small nodules in the thyroid gland. The enlargement can be very subtle, so that it can only be seen by measuring in the ultrasound or with the head leaning back strongly or is even visible in a normal posture and can cause swallowing difficulties.
In extreme cases, the enlargement can even narrow the trachea, which is located directly behind the thyroid gland, causing shortness of breath. If the enlargement is also painful, then an inflammation of the thyroid gland (= thyroiditis) must also be taken into account. It is important to know that the size does not say anything about the hormone production. People with a large thyroid do not automatically have high levels of thyroid hormones in their blood. Quite the opposite: it is not uncommon for people to be underfunction.
At 90%, iodine deficiency is the most common cause of the painless enlarged thyroid gland. The lack of iodine in the body is mostly due to a lack of iodine in the diet. Iodine deficiency leads to a deficiency of thyroid hormones in the body, because iodine is a key component of these hormones. The thyroid, like many tissues in the body, reacts to this deficiency by growing its tissue so that it can produce hormones more effectively. However, this growth does not take place equally strongly at all points of the thyroid gland and it comes to the formation of differently active areas, the "node“.
In the case of iodine deficiency, the administration of iodine tablets or, rarely, additional “finished” thyroid hormones, often leads to the thyroid gland shrinking and the abnormally grown areas recede. In addition to the iodine deficiency are Autoimmune diseases rarer causes of thyroid growth such as M.Basedow (= Basedow's disease) or Hashimoto's thyroiditis (named after the Japanese doctor Hashimoto). Here the body reacts to the thyroid tissue, because it no longer recognizes it as belonging to itself and attacks it. This attack changes the metabolism of the thyroid gland and leads to the growth of all thyroid tissue. A cyst (fluid-filled cavity) or certain medications (e.g. lithium or nitrates) can also lead to enlargement.
In any case, an enlarged thyroid gland must be clarified in detail, as a tumor can rarely be the cause of the enlargement. Only when the exact cause of the enlargement is known can the correct treatment of the enlarged thyroid gland be started, which varies greatly depending on the cause.
Read more on this topic at: Thyroid Enlargement
Thyroid Removal
An operation is only necessary for certain findings or a certain combination of findings. Here, too, there are differences in how the operation is carried out. Either only parts of the thyroid gland (=Lobectomy) or the whole thyroid gland (=Thyroidectomy) remove. The ear, nose and throat doctor is often responsible for this, as he has the greatest experience in performing operations in the neck area. The operation is usually associated with a two to three day hospital stay.
In most cases, it is people who have lumps in the thyroid gland who will need surgery. So-called "Cold" knots almost always have to be removed, as they must be examined under the microscope because they could be malicious in nature, even if this is rarely the case. However, if the suspicion is confirmed, it is a complete one distance of the thyroid gland, because this is the only way to guarantee the complete removal of the tumor and reduce the risk for one Relapse (= Recurrence) should be reduced as much as possible. The "to warm"Or"be called“Nodules are usually removed when they impair thyroid function and thyroid function can no longer be controlled by medication.
Removal should also be considered if the enlargement causes problems when swallowing or if it affects neighboring organs such as the windpipe. The need to clear their throat or the constant feeling of a foreign body in the throat are also not infrequently the reasons why those affected decide to have surgery. This is an important alternative to surgery Radioiodine therapy. Here the thyroid is slowed down by swallowing a capsule of radioactive iodine, which mainly damages the very active producing cells, as these absorb most of the radioactive substance. Whether surgery, radioiodine therapy or even administration of medication alone is considered depends on the individual case and must be decided individually for each patient.
The most serious consequence of thyroid surgery, especially its complete removal, is the loss of its function. Since thyroid hormones are vital, they must be replaced in tablet form. If they are not replaced enough, our physical development and performance as well as our overall mental wellbeing are impaired. The hormones must be taken in the correct dosage for the rest of life, which requires regular blood tests.
It is also very feared Vocal cord paralysis, because the nerve responsible for the vocal cords (lat: Recurrent laryngeal nerve), which controls this, runs precisely through the operating area along the thyroid gland. Although the nerve is carefully spared and monitored very carefully during the operation, damage cannot be ruled out that would result in temporary or permanent vocal cord paralysis. For those affected, this means a permanently hoarse voice and the loss of the ability to sing. In very serious cases, in which both nerves (right and left of the neck) are affected, shortness of breath can result as the Vocal folds can no longer open due to the paralysis.
A larynxoscopy can then clarify the findings. Structures that must be carefully observed during the operation are the same Parathyroid glands. These 4 small bodies sit on the thyroid gland only separated by a thin layer of tissue. They produce the so-called Parathyroid hormone, what influence on the Calcium metabolism our body has. If they are removed during the operation, the calcium balance gets into a complete mess and it can become too Muscle spasms or tingling in your arms or legs. Similar to the thyroid hormones, however, the parathyroid hormone can also be taken as a tablet.
Pain (causes)

Swelling in the neck, pain in the area of the thyroid gland and pain when pressure is applied to it, redness and overheating: these can all be signs of thyroid inflammation (= Latin: thyroiditis; the ending -itis describes the inflammation).
Inflammation of the thyroid gland is one of the rare diseases of the thyroid gland. However, not all inflammations are created equal; there are different forms here too. The classification is based on various criteria.
On the basis of the temporal course, one differentiates between the acute, the subacute or the chronic Inflammation of the thyroid gland. The acute inflammation starts very suddenly. The cause are usually infectious agents such as bacteria or fungi that strand in the bloodstream in the thyroid gland, which is well supplied with blood, and lead to inflammation there. Most of those affected report a previous infection such as tonsillitis, followed by increasing swelling and pain in the thyroid gland. The affected areas on the neck are red and the patients complain of difficulty swallowing, fever and feelings of illness.
Radiation as part of tumor therapy or certain medications also lead to inflammation of the thyroid. The less sudden form (subacute thyroiditis) is probably caused by viruses such as the mumps or measles viruses. The course is variable and can show any appearance from no symptoms to the extent of the acute form. The magnification is usually limited. The onset is usually up to two weeks after the infection and patients complain of tiredness and exhaustion.
The long-lasting chronic form is usually triggered by autoimmune diseases, that is, the body no longer recognizes the thyroid gland as a part of itself and begins to fight it like any "enemy" with markers (so-called antibodies).
The antibodies mark the apparently foreign tissue and various body cells then lead to the destruction of these structures marked as foreign according to their task. The most well-known disease of these autoimmune diseases is Hashimoto's thyroiditis.
The inflammation progresses very slowly and those affected often only become aware of their disease through the increasing hormone deficiency. An HIV disease is also very rarely the cause of the chronic inflammatory reaction.
Hyperthyroidism
An overactive thyroid is also known in technical terms as hyperthyroidism.
This is a disease that is associated with increased production of the thyroid hormones thyroxine (T4) and triiodothyronine (T3).
The prevalence of hyperthyroidism is 2-3% of the total population. In Germany, the most common causes are the autoimmune disease Graves' disease or functional autonomy of the thyroid gland. Between the ages of 20 and 40, Graves' disease is the most common cause of hyperthyroidism, but from the age of 50 onwards, functional autonomy.
The symptoms of hyperthyroidism are very diverse. The increased hormone production mainly affects the metabolism and circulation, but psychological well-being and growth are also influenced.
In general, patients often complain of nervousness, restlessness, insomnia, increased sweating, and weight loss. In addition, it can lead to hair loss, increased appetite and thirst, increased stool frequency with possibly diarrhea and muscle problems (Myopathy) come. In rare cases, male patients with an overactive thyroid can develop gynecomastia (Enlargement of the mammary gland) train; Women also complain of menstrual disorders. A characteristic finding of immunologically induced hyperthyroidism is pretibial myxedema (= swelling of the skin on the shin bone due to the storage of glycosaminoglycans).
The therapeutic treatment of hyperthyroidism is usually medication with so-called thyreostatics. These drugs use different mechanisms to inhibit the new synthesis of thyroid hormones with the aim of achieving euthyroidism (= normal thyroid production). The overactive thyroid can also be treated surgically. The prerequisite, however, is the euthyroid metabolic status before the start of the operation using thyreostatics.
Follow-up care with L-thyroxine is then mandatory, as the partial resection (removal of certain parts) of the thyroid gland can result in hypothyroidism, i.e. underfunction. A frequent undesirable complication during surgery is injury to the recurrent laryngeal nerve (recurrent palsy), as it has a close topographical relationship to the thyroid gland.
Read more on the topic: Hyperthyroidism
Cold knot

Nodules in the thyroid gland can be found in over 50% of the population and the proportion increases with age. Studies have shown that from the age of 65, a lump can be found in every second adult. In addition to cysts (fluid-filled cavities), growths, scarring and calcifications, nodes can also represent hormone-producing altered thyroid tissue. In medical terminology, a distinction is made in relation to the hormone-producing nodes "cold“, „warmth" and "name is“Knot from each other. The term cold, warm or hot, however, is not about the temperature of the node, but about its activity, i.e. whether or not they are diligently producing hormones.
This hormone production can be measured using what is known as scintigraphy. A colorful image of the thyroid is made with the help of different colors. The activity of the area determines the color in which it is displayed on the image. The colors in the hot, very active areas change to warm tones such as red and yellow and to cold colors such as blue and green when activity is reduced. Behind such an area of a cold lump there is often a simple change in tissue that is no longer able to produce hormones. These can be cysts (fluid-filled cavities), adenomas (benign growths of hormone-producing cells), calcifications or scars in the tissue.
Read more on the topic: Cold lump on the thyroid gland
In rare cases (max. 5%), however, a malignant tumor can also be behind it. In advance, rapid growth and a coarse, immovable consistency can indicate malignant growth. A cold lump always needs treatment because of this rare cause.
A final diagnosis can be made with a fine needle aspiration, an uncomplicated type of biopsy. A small tissue sample is taken through a thin needle and examined under the microscope. Depending on whether the change is good or bad, the procedure for treatment differs from observation through regular ultrasound checks to complete removal of the thyroid gland.
Find out more at: Thyroid biopsy
Radioiodine therapy does not work on cold lumps. Since the procedure is based on the cells absorbing radioactive iodine and these nodes absorb little iodine, the cells cannot be combated and the therapy cannot have any effect.
Hot knot
Hot knots are common in our civilization. They often arise from the extensive iodine deficiency in the population. This deficiency leads to the decreased production of Thyroid hormones, because the cells of the thyroid are dependent on it. Since the body needs the hormones anyway, it releases growth factors so that the thyroid gland grows and hopefully produces more hormones again. If this happens unevenly across the thyroid gland and one area grows more than another, a hot lump develops.
However, not all thyroid nodules can be prevented even with sufficient iodine intake. This suggests that genetic changes can also lead to the formation of knots. Warm and hot lumps are only very rarely malignant; they cause those affected mainly problems due to excessive hormone production. The areas in the node that have grown above average are less sensitive to the body's signals and, regardless of the signals, always produce an excess of hormones and so-called Overactive thyroid (Hyperthyroidism) with an autonomy (= self-determination) of the node.
This excess can partly be compensated by the fact that other areas reduce their hormone production, but this also has its limits and sooner or later the excess can no longer be compensated. This excess turns the body upside down, it works at full speed: the heartbeat accelerates and can become irregular, you are restless, nervous and sweat, you lose weight and have digestive problems. This overproduction can be tried with slowing drugs, so-called Anti-thyroid drugs,, to keep in check. If this does not succeed, an operation or radioiodine therapy is the method of choice here too, because in the long run this condition is harmful to the body, as it cannot work at full speed all the time, causing long-term damage to various organs, especially Nervous system and Cardiovascular system, can follow.
Patients with hot lumps can go through exams with X-ray contrast media get into a life-threatening situation. There is an enormous amount of iodine in X-ray contrast media. If this reaches the thyroid gland through distribution in the bloodstream during the examination, the iodine is immediately absorbed by the very productive areas in the node and converted into hormones. These now flood the blood and life-threatening occurs Thyrotoxic crisis, by Racing heart and Arrhythmia can be fatal.
In the case of necessary examinations in which the contrast agent is absolutely necessary, those affected can be treated with a protective drug, Perchlorate, to be protected. This prevents life-threatening hormone production and the examination can be carried out safely.
Goiter
The enlargement of the thyroid gland with proper hormone production is called "Goiter"(Synonym: Goiter). The thyroid is considered enlarged if it exceeds a volume of 18ml in women and 25ml in men.
A goiter can be due to a hereditary defect, existing iodine deficiency, so-called "strumigen“Substances (for example Nitrates, lithium or Thiocyanate) arise in food or certain medications. The most common cause is iodine deficiency. Since Germany is considered an iodine deficiency area, it is understandable that more than 30% of the population suffer from an enlarged thyroid. Women are affected roughly twice as often as men.
The iodine deficiency induces the release of in the thyroid gland Growth factors, which then increases the size of the thyroid cells (=Hyperplasia) and cause the surrounding connective tissue to grow. The more the iodine content falls below the optimal value of 200µg, the more the thyroid gland is stimulated to grow.
In addition to the iodine deficiency, there are other factors that can cause goiter; these include the Autoimmune diseases (M. Basedow and Hashimoto), Thyroid autonomy, Inflammation of the thyroid gland (Thyroiditis), one Hyperthyroidism and last one Thyroid cancer.
In principle, a goiter can be treated conservatively and medically.To compensate for the iodine deficiency, patients receive an iodine substitution (100-200 µg / day). If necessary, a combination therapy with thyroxine (50 µg / day) is also carried out if there is insufficient improvement, as both reduce the growth stimulus. Surgical therapy is only indicated if cancer is suspected or goiter with autonomies. Depending on how severe the suspicion is, there is a partial or total resection (distance)
One complication in those with goiter is that Formation of nodular substances, so-called "hot or cold knots". This leads to a transformation of the diffuse struma tissue with a simultaneous loss of controllability by the hormone TSH, which triggers thyroid hormone production.
To prevent a goiter, it makes sense to prophylactically (precautionary) to be treated with iodine tablets.