Supraspinatus tendon
Location and function
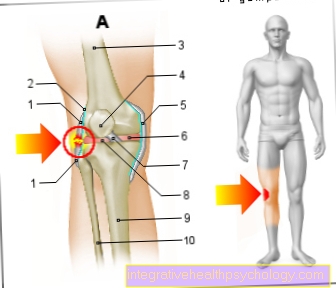
The supraspinatus tendon is the insertion tendon of the supraspinatus muscle (upper bone muscle). This muscle has its origin on the back of the shoulder blade and attaches to the head of the humerus via its tendon. The muscle is primarily responsible for spreading the arm away from the body (especially from an angle of more than 60 °) (abduction). Together with three other muscles (infraspinatus muscle, subscapularis muscle and teres minor muscle) it forms the so-called rotator cuff. This muscle group also serves to rotate the upper arm (inside and outside), but its most important task is to stabilize the shoulder joint, which is otherwise relatively free to move and not very secure.

Illnesses and injuries
Because the supraspinatus tendon is in an anatomically close relationship to Bursa and the shoulder roof (Acromion), it is particularly prone to injuries and is therefore a common cause of Shoulder pain. There are three typical clinical pictures in the foreground: Impingement syndrome, Calcifications (which can very often be caused by degenerative changes) and the Rotator cuff rupture, in which the supraspinatus tendon tears off particularly often.
At the Impingement syndrome there is not enough space in the shoulder joint for all structures, which is why certain parts of the joint collide unnaturally and cause pain for the person affected. This sometimes severely restricts the mobility of the shoulder joint. This can have very different causes, but the most common cause of this bottleneck is that the supraspinatus tendon is thickened. This can be for various reasons: Either it has been exposed to long-term overload or it has swollen as a result of inflammation or degenerative changes. When the arm is spread sideways, the supraspinatus tendon always migrates towards the middle of the body and slides between the Humerus head and the Shoulder roof.
If this is now thickened, however, the area under the roof of the shoulders (the subacromial space) is reduced too much and the structures in it are narrowed. This means that tendons rub directly against each other or against the bones or the bursa, thereby irritating different tissues. This leads to pain, especially when the arm is abduced between 60 and 120 °, which is why this disease is also referred to by some as a "painful arch". In some cases, the pain can extend well into the upper arm radiate and may also persist at night when the person concerned turns over on the diseased side. Operationally a Impingement syndrome usually treated well.
Rotator cuff rupture is more common with impingement syndrome, but it doesn't necessarily have anything to do with it. In the course of life, the supraspinatus tendon becomes thinner and less resistant to tears due to constant stress. This is caused by the natural wear and tear of the tendon and, in part, by the resulting degenerative changes. Once the tendon is so “thinned out”, it can easily happen that it is so overused, even as a result of minimal violence, injuries or accidents, that it tears or even tears off.
In major accidents, such as a fall that is caught by the outstretched arm, a previously undamaged tendon can tear. The complaints a patient complains about are, depending on the extent of the tear, pain, restricted mobility (especially with abduction and external rotation) and a reduction in strength. If the tendon is not completely severed, the rupture is usually followed by conservative therapy (with medication and physical therapy) at. This does not restore the tendon, but normal everyday use can usually be restored within a short period of time. If it is unsuccessful or if the tendon is completely torn off, there is usually no way around having an operation performed.
Another common disease of the supraspinatus tendon is tendinosis. Tendinitis calcarea, i.e. a calcification of the tendon or the tendon attachment. Here calcium deposits develop either under or on the tendon itself, which in turn causes the tendon to become inflamed. This inflammation then brings the typical signs of inflammation with it, especially pain, swelling, reddening and restricted movement of the shoulder joint. The exact cause of these changes could not be finally clarified until today, they are only partly degenerative (i.e. a form of arthrosis), but sometimes they occur without any recognizable reason. With help of a X-ray image the calcifications can be seen well and the diagnosis is relatively easy to make.
Since the pain can become very severe and calcification can often lead to a rupture of the supraspinatus tendon at some point, therapy is usually recommended. Depending on the patient, this therapy can be conservative (i.e. with cooling, medication, physiotherapy or recently the so-called Extracorporeal shock wave therapy [ESWT], in which the calcium deposits in the shoulder are shattered from the outside by low-frequency shock waves, which, however, is still controversial despite good results) or in more severe cases by an operation in which the calcifications are removed. Unfortunately, even after an operation, the relapse rate is not to be despised, and calcifications also lead to spontaneous healing, which is why the pros and cons of performing an operation must always be carefully considered by the doctor and the patient.
Inflammation of the supraspinatus tendon
Due to its location and the stress it is exposed to, it can come back to one quickly and again inflammation in the area of the tendon of the supraspinatus muscle. Most of the time, such inflammation is caused by a Overuse of muscles in the shoulder area (e.g. lifting to heavy loads) or by a Improper loading (incorrect lifting of loads).
Symptoms an inflamed tendon of the supraspinatus muscle are mainly stabbing or biting pain when lifting or turning the arm with partial loss of strength and fine motor skills. The most important measure in this context is first of all that Avoid this type of exercise. You can also try to use cooling take action against the pain. If these measures are not sufficient, a anti-inflammatory pain therapy in the form of Ibuprofen or Diclofenac respectively.
If the tendon is inflamed again and again, it should be partly therapeutic and partly preventive Treatment by the physiotherapist respectively. It helps to train the other muscles accordingly, i.e. to relieve the tendon of the supraspinatus muscle. Can also Use of a kinesio tape be useful. An elastic adhesive tape is stuck to the natural course of the supraspinatus muscle and is intended to ensure that the muscle is relieved and its movement is spared.
Calcified supraspinatus tendon

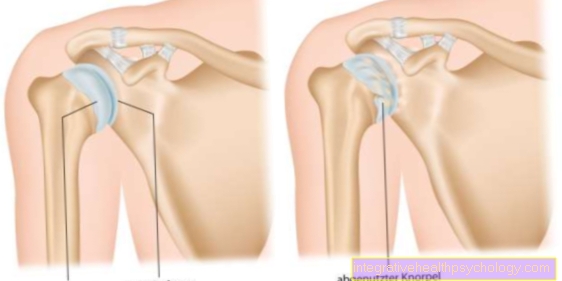
The supraspinatus tendon extends over the head of the humerus of the shoulder joint and is responsible for numerous movement, holding and stability processes in the shoulder area. It is exposed to many frictional and shear forces every day. As with any mechanically stressed fabric, the body tries to prevent corresponding signs of wear and tear, which it tries to do by thickening the fabric. On the one hand, it makes sense and on the other hand it also causes further discomfort, the body deposits lime in heavily stressed areas of the supraspinatus tendon, which is supposed to serve as protection and stabilization. This phenomenon is also known as the calcareous shoulder.
Since the space situation in the shoulder joint is very limited, this tendon thickening quickly leads to a space problem: surrounding tissue, nerves and tendons of other muscles rub against the increasingly cold supraspinatus tendon, which also triggers friction processes through its own movement. This tight space situation triggers irritation of the supraspinatus tendon, which, if the movements are not reduced, can also become inflamed. The patient describes drawing, biting pain when moving.
Once the diagnosis has been made, the therapy of choice is primarily the temporary immobilization of the arm as well as cooling and anti-inflammatory pain treatment. If the symptoms become chronic, a jointoscopy with removal of the calcifications should be considered.
Read more on the subject below Lime shoulder
Supraspinatus tendon rupture
In the event of a tear in the supraspinatus tendon, also known as a Rotator cuff tear The supraspinatus tendon is suddenly separated from the muscle or the tendon is divided into two halves. Although the demolition suddenly and mostly after a jerky movement of the arm or after the Lifting a heavy last occurs, a distinction is made between an acute and a chronic form as the cause.
In the acute form it comes to one completely intact tendon by a too heavy lifting movement or by a wrong movement, to one suddenly the tendon ruptured. In the chronic form it comes from incorrect loads that have taken place over many years with the resulting Degeneration of the tendon to a weakening of the muscle. Most of the time, a heavy weight is no longer necessary before it can tear off.
The actual demolition is with sharp, sharp pain connected, sometimes an instantaneous one occurs Restriction of mobility in the area of the affected shoulder. Treatment takes place in the vast majority of cases operational. Sometimes also conservative. Through a arthroscopic surgery, the two ends of the tendon are brought closer together and sutured. The healing takes place over several weeks under one Follow-up treatment of the rotator cuff tear With physiotherapeutic strength building.
Taping the supraspinatus tendon
The supraspinatus muscle is one of the strong muscle group of the shoulder muscles and is responsible for the movement and stability of the upper arm in the shoulder joint. The tendon of the muscle runs between the humerus head and the shoulder roof and encloses the shoulder head. Because of its stretching position, the supraspinatus tendon is especially often of heavy use and also Degeneration affected.
This is a therapy for this resulting pain physiotherapy tapes the area of the tendon. In this non-surgical measure, a elastic adhesive tape (Kinesio tape) glued to the course of the muscle of the supraspinatus muscle. The tape should, if possible, over a period of worn continuously for several days become. It acts as a passive muscle substitute and promotes one stability in the shoulder joint, a regulation of muscle tone, a Anti-inflammatory as well as a reduction in swelling.
Appointment with a shoulder specialist

I would be happy to advise you!
Who am I?
My name is Carmen Heinz. I am a specialist in orthopedics and trauma surgery in the specialist team of .
The shoulder joint is one of the most complicated joints in the human body.
Therefore, the treatment of the shoulder (rotator cuff, impingement syndrome, calcified shoulder (tendinosis calcarea, biceps tendon, etc.) requires a lot of experience.
I treat a wide variety of shoulder diseases in a conservative way.
The aim of any therapy is treatment with full recovery without surgery.
Which therapy achieves the best results in the long term can only be determined after looking at all of the information (Examination, X-ray, ultrasound, MRI, etc.) be assessed.
You can find me in:
- - your orthopedic surgeon
14
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
You can find more information about myself at Carmen Heinz.