Lymph node cancer
introduction
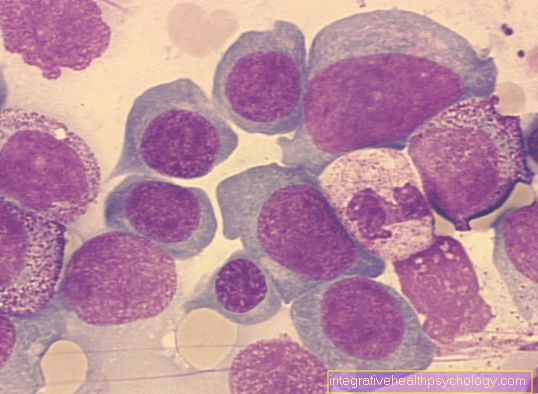
Lymph node cancer - better known as lymph gland cancer or lymphoma - is a malignant tumor disease in which lymphatic cells degenerate: some of the white blood cells (the Lymphocytes), which are usually included in the Immune defense involved have changed so much that they are theirs lose their original function and yourself multiply unchecked.

At the beginning of the disease, in the early stages, it is usually a local occurrence, since the degenerated lymphatic cells are usually only found in one or more lymph nodes and initially persist in a spatially limited manner. Only in the advanced stage, i.e. in the course of the disease, are other areas of the body also affected: by spreading or spreading (metastasis) the degenerated cells reach the lymphatic and / or blood vessel system from the affected lymph nodes to other organs and a local tumor disease becomes a malignant systemic disease. Organs such as the skin, liver, bone marrow and kidneys can then be affected. In principle, lymph gland cancer can be divided into two groups, which differ from one another in terms of definition, underlying cause, clinical picture and prognosis:
25% of all lymphomas make the so-called Hodgkin lymphoma (Hodgkin's disease), the rest 75% put the Non-Hodgkin lymphoma represent.
Stages classification
Lymph node cancer or lymphomas can be identified using the so-called Ann Arbor Classification in four different stages organize:
- Stage 1: 1 lymph node region is infected or 1 extranodal Focus (settlement of degenerate cells not affecting the lymph nodes) is detectable.
- Stage 2: More than 2 Lymph node regions on one side of the The diaphragm is affected or 1 extranodal focus + 1 lymph node region on one side of the diaphragm can be detected.
- Stage 3: More than 2 Lymph node regions over both sides of the diaphragm are affected or several extranodal foci + more than 1 lymph node region over both sides of the diaphragm are detectable.
- Stage 4: on the whole body distributed organ involvement with or without lymph node involvement
Causes of Lymph Node Cancer
Both Hodgkin lymphoma is it a Degeneration of the B cells of lymphocytes, although the underlying cause is in most cases unknown. A connection with an existing infection with the Epstein-Barr virus is suspected (EBV). An existing one comes as a risk factor immunodeficiency in question (e.g. with a Immunosuppressive Therapy or HIV infection).
From the Hodgkin lymphoma are more men than women affected, the 3rd and 5th decade of life as the main age of manifestation be considered.
Both Non-Hodgkin lymphoma it is, however, about degeneracies that from both the B and T cells of the lymphocytes can go out. Also here are more men affected, with the likelihood of getting sick increasing age increases. The trigger for non-Hodgkin lymphoma is also often unknown, only different risk factors are clearly known: besides one family history and one existing genetic modification (Chromosomal aberration), also count ionizing rays (e.g. X-rays), chemical poisons, Immune system disorders (e.g. HIV) and certain Infections (e.g. EBV, HTLV-1) are among the factors that can promote non-Hodgkin lymph node cancer.
Symptoms of lymph node cancer

Even at the onset of lymph node cancer, the affected lymph nodes are noticeable in both Hodgkin's disease and non-Hodgkin's lymphoma: they are usually enlarged but not tender on pressure and can no longer be moved relative to the subsurface (enlarged lymph nodes in A cold or infection, on the other hand, is usually painful and changeable!).
The most common lymph nodes in Hodgkin's disease are in the area of the Head and neck area affected (60% on the neck), but less often Lymph nodes in the Armpit area (20%) or Groin area (10%).
The affected region in non-Hodgkin lymphoma is somewhat less specific.
Both types of lymph node cancer are in most cases caused by what is known as B symptoms accompanied by a inexplicable fever above 38 ° C, profuse sweating while sleeping and one unwanted weight loss is characterized by over 10% of body weight in the last 6 months.
It can also have a strong feeling of being Exhaustion and fatigue to be added as well as in Itchy skin in 25% of cases over the entire body.
Pain in the affected lymph node region is rare, but particularly important for Hodgkin's disease after drinking alcohol and the so-called Pel-Ebstein fever (Fever lasting 3-7 days, which alternates with fever-free intervals).
Read detailed information on the topic: Pel-Ebstein fever
There is also one for both types increased susceptibility to infections due to the attacked immune system.
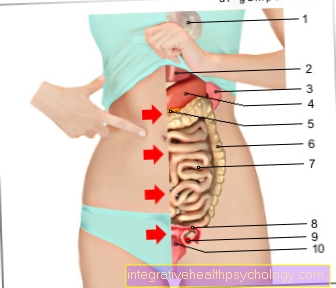
In the advanced stage, organ systems outside the lymph nodes can also be affected, so that a. to a enlargement liver and spleen and bone marrow involvement with changes in blood formation and neurological symptoms.
Diagnosis of lymph node cancer

For both types of lymphoma, a physical examination can provide initial indications, as the affected lymph nodes are often enlarged and hardened and palpable.
A precise blood test is then essential for further clarification. In many cases, anemia (anemia), a lack of lymphocytes (Lymphopenia; Attention: from case to case, however, there may be an excess of lymphocytes!) And a lack of blood platelets (Thrombocytopenia) prove. Furthermore, the sedimentation rate is oftenBSG) and the LDH value increased, the value of blood protein (Serum albumin) but lowered.
If, on the basis of the physical examination and the blood count, the suspicion that it may be a lymph node cancer, a lymph node biopsy of the affected lymph node region is arranged to then examine the degenerated tissue of the lymph nodes histologically and to confirm the diagnosis can.
Read more on the subject at: Lymph node biopsy
Here, either a sample is taken from the lymph node tissue (using a biopsy needle or punch) or even the entire lymph node via a skin incision under local or general anesthesia.
Once the diagnosis has been finally confirmed, it is necessary to determine the complete extent of the tumor in the body in order to determine the tumor stage, the best possible therapy and the prognosis.
For this purpose, so-called Staging exams These include an ultrasound scan of the abdomen and lymph nodes in the armpit, neck, and groin area, chest x-ray and CT scan, skeletal scintigraphy, and bone marrow and liver biopsy.
Therapy for lymph node cancer
The goal, both in the treatment of Hodgkin's disease and in the treatment of non-Hodgkin's lymphoma, is one Cure or contain the disease in all four stages described above.
In general, chemotherapy and radiation therapy are available as forms of therapy, with radiation therapy usually following chemotherapy.
In the stadium 1 and 2 of the Ann Arbor Classification will be initially two cycles of chemotherapy performed, which is usually a combination of several chemotherapeutic agents (ABVD: Adriamycin, Bleomycin, Vinblastine, Dacarbazine). This is followed by a so-called Involved field irradiation, radiation is strictly limited to the affected region in order to protect the surrounding healthy tissue.
in the Stage 3 and 4 will be in the Usually 8 cycles an extended chemotherapy performed (combined chemotherapeutic agents: Bleomycin, Etoposide, Adriamycin, Cyclophosphamide, Vincristine, Procarbazine, Prednisolone (BEACOPP)), which is then also replaced by a Involved field irradiation supplemented if residual tumor tissue can be detected after chemotherapy.
The therapy of non-Hodgkin lymphoma depends on the Degree of malignancy. Severely malignant non-Hodgkin lymphomas usually respond well to chemotherapy, regardless of the stage (CHOP therapy regimen: Cyclophosphamide, Hydroxydaunorubicin, Oncovin (Vincristine), Prednisolone). If there is evidence of residual tumor tissue, this is also done here post-irradiated. Non-Hodgkin lymphomas, on the other hand, which are less malignant, respond very poorly to chemotherapy because of their slow growth.
In stages 1 and 2 - with a prospect of healing - they are only irradiated on their own or in some cases even left untreated under observation.
In stages 3 and 4 a cure is usually no longer possible, but chemotherapy according to the CHOP scheme is nevertheless attempted if the symptoms are very pronounced.
Prognosis and course in lymph node cancer
The prognosis of Hodgkin's lymphoma differs significantly from that of non-Hodgkin's lymphoma. However, the prognosis is dependent on both cases of the existing stage and the timein which the appropriate therapy is initiated.
Due to the expansion and improvement of therapy in recent years, the prognosis of an existing lymph node cancer has improved a lot, so that the chances of recovery are good in many cases.
The so-called 5 year survival rate at Hodgkin's disease is currently included approx. 80-90%which means that 80-90% of affected patients are still alive after 5 years. The fact that the 5-year survival rate is over 90% in the initial stage, but is still 80% in the advanced stage, shows that Hodgkin's disease still has good chances of recovery in the later course of the disease.
However, it is relatively high Recurrence rate, so the probabilitythat Hodgkin's disease comes back after a certain time.
Also exists with a 10-20% probability the possibility of a second, different cancer to suffer from lengthy chemotherapy and radiation therapy.
Both Non-Hodgkin lymphoma the prognosis also depends significantly on the Degree of malignancy (the degree of malice) from. Non-Hodgkin lymphoma types, which tend to be less malignant and tend to occur in old age, are difficult or impossible to heal, but they can usually be because of their slow growth over a period of well controlled for up to 10 years become.
Non-Hodgkin lymphoma types, however highly malignant have a Long-term healing prognosis of up to 50-60% (If left untreated, however, they very quickly lead to death).