Elbow dislocation
Synonyms: elbow dislocation, elbow dislocation, elbow dislocation
definition

An elbow dislocation is a complete displacement of the parts involved in the elbow joint. This includes sliding out of the joint surface of the humerus (Humerus) from its hinge-like enclosure by the ulna (Ulna) and the loss of contact between the head of the spoke (radius) and the humerus.
anatomy
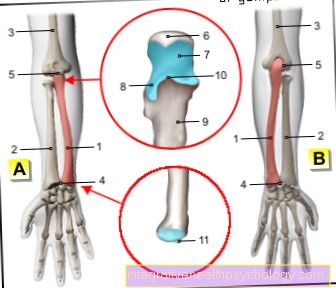
In the elbow joint (Articulatio cubiti) three bones meet: the humerus (Humerus), the cubit (Ulna) and the spoke (radius). They form 3 different joints among themselves, which together form a so-called rotary hinge joint (Trochoginglymus) result.
The humerus has a rounded articular surface, which is hinge-like around the ulna with two bone processes (hinge joint). These projections are at the back as "Elbow bones"Palpable upper end of ulna (Olecranon) and in front the crown process (Proc. Coronoid).
The head of the spoke (Caput radii) surrounds a spherical joint surface. This laterally forms a swivel joint with the ulna, which is supported by a circular band running around the head of the spoke (Annular radial ligament) is stabilized. Upwards, the spoke head forms a ball-and-socket joint with the joint surface of the humerus.
The lateral movements of this ball joint, however, are restricted on both sides by collateral ligaments between the humerus and the radius or ulna (Ligamentum collaterale radii or ulnae).
The joint capsule is relatively wide and includes the joint-forming parts. Muscles and the collateral ligaments attach there and additionally stabilize the joint.
A healthy joint allows an outward rotation (Pronation) and inward rotation (Supination) of the forearm and a flexion of about 140 °. A further extension beyond the resting position is not possible due to the bony structures (except for women and children sometimes 5-10 °). Lateral kinking of the forearm is also not possible with intact ligaments.
Emergence
The Elbow dislocation can rarely be congenital, but is in almost all cases external Violence conditionally.
The most common mechanism is that Fall on the outstretched arm, this situation often occurs in sports. Direct effects on the arm can also be the cause, if a Hyperextension or a excessive angling in the elbow joint.
According to the high proportion of falls on the outstretched arm, there is one in about 80-90% of cases dorsal (back) dislocation: Due to the force applied from the front, the upper end of the ulna (olecranon) becomes a pivot and lever the humerus out of its joint pit. As a result, it is located in front of the actual joint. However, the ulna and radius are located behind the humerus, which is crucial for classification as a dorsal dislocation.
In less than 10% of the cases one occurs sole (isolated) dislocation of the spoke head from its position. In even fewer cases, after the dislocation, the ulna and radius are located in front of (ventral) or next to the humerus or are located separately from each other on one side (diverging).
The elbow dislocation always has one Tearing the capsule result. It also occurs in many cases Damage to the ligament apparatus, for example torn ligaments on the elbow. In about 20% of the cases Dislocation of accompanying bony injuries to.
This can be the fracture of the head of the spoke, the tearing off of the crown process or the upper end of the ulna (olecranon) or tears of the humerus. Also Injuries to the ducts (Arteries, veins, nerves) occur because these run in close proximity to the elbow joint.
Appointment with an elbow expert?

I would be happy to advise you!
Who am I?
My name is I am a specialist in orthopedics and the founder of .
Various television programs and print media report regularly about my work. On HR television you can see me every 6 weeks live on "Hallo Hessen".
As a former performance-oriented tennis player, I specialized early on in the conservative treatment of the elbow.
You can find me in:
- - your orthopedic surgeon
14
Directly to the online appointment arrangement
Unfortunately, it is currently only possible to make an appointment with private health insurers. I hope for your understanding!
Further information about myself can be found at
therapy
In general, the joint should be corrected as soon as possible, preferably within 6 hours. Otherwise there is a risk of vascular or nerve damage due to the spatial proximity.
In the case of a dislocation without accompanying bony injuries, the goal is reduction, the restoration of normal joint conditions. To do this, the joint surface of the humerus must snap back into the joint pit of the ulna. This is usually carried out under general anesthesia, since with regional anesthesia the feeling and the ability to move are restricted for a long time, which can be dangerous.
In the case of a dorsal dislocation, with the upper arm fixed, a pull is exerted on the forearm, which is flexed by approx. 30 ° and rotated outwards, and this is bent to 90 °. In the case of ventral dislocation, the forearm is bent and an attempt is made to snap it back into place. After the reduction has taken place, the joint must be checked by x-rays.
If ligament damage is suspected, the success of the reduction and the extent of the remaining instability of the joint should be assessed during the anesthesia. When the patient is awake, muscles attached to the joint can simulate stability. The verification is controlled by simultaneous rapid sequences of X-rays. Above all, it is important to check how the joint behaves when it is bent and bent outwards or inwards. If there is no renewed dislocation, treatment is conservative with a 1 to 2 week plaster immobilization in the functional position (approx. 90 ° flexion). If there is an instability in relation to the kinking outwards or inwards, this time can be increased to 3 weeks. However, physical therapy should be started as soon as possible to prevent capsule shrinkage and muscle hardening.
If during the functional check, especially when bending, a new dislocation occurs (Reluxation), or if the joint cannot be repositioned at all, surgery is indicated. Likewise, if instability persists after conservative treatment (immobilization). Surgery must also be performed if there is bone damage or nerve and vascular damage. Here, the joint is repositioned, the bony structures are fixed in their original arrangement and the capsular ligament apparatus is restored. A is often used to fix the joint and its parts External fixator for use. The bony parts are fixed through the skin with screws. There is also a so-called Motion fixatorthat allows movement within a specified range. The advantage is that movement training can be started earlier. Movement restrictions as a long-term consequence are to be minimized.
Read about this too Elbow brace
Complications
To the Complications belong in about 10% of cases Injuries to the vessels. Especially with arterial vessels, this is due to the high blood pressure prevailing there acute emergency. Also Injuries to the nerves (Ulnar nerve, median nerve, radial nerve) with paralysis of the muscles and loss of touch sensation in typical areas occur.Dislocation occurs in a not inconsiderable number of cases Calcifications or. Ossification of connective tissue (heterotropic ossification). If these restrict movement, they can surgically removed become. It should be remembered that the operation itself can trigger the same phenomenon.
For prevention, pain relievers such as indomethacin or Diclofenac (Voltaren©) given.
forecast
At a simple dislocation treated conservatively without accompanying damage is a full recovery (Restutio ad integrum) expected. Reluxation occurs in around 2 out of 100 cases.
The more complex the injury, the longer it will take to heal and the more likely it is Late damage. This usually includes one stiffness with more restriction on extension than on flexion. In the event of damage to the spoke head and its stabilizing band (Annulare radii) are Limitations of rotation of the forearm to be expected.
2% of all patients develop one after an elbow dislocation chronic instability with repeated dislocations. The cause is usually the lack of stability of the joint-guiding structures after bone fractures.